Five questions kidney patients should ask before taking a new medication
By Majd Isreb, MD, FACP, FASN, IFMCP
Is it necessary?
There are many instances when a medication may be inappropriate—for example, using an antibiotic for a viral infection. However, with the short time providers spend with their patients, it is not uncommon to see medication being prescribed before any attempt at lifestyle modifications. Lifestyle modifications should be the first step in the management of many chronic diseases. This includes educating patients and coaching them on these modifications for at least six months.
Does it harm the kidneys?
Many medications can cause direct or indirect harm to the kidneys, and every day there is a newer medication on the market. Sadly, some providers may not be aware if a drug being prescribed is harmful to the kidneys or not. It is, therefore, necessary for the patient to ask themselves and their provider that question.
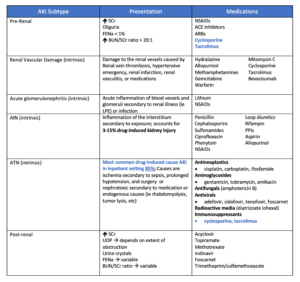
The following table shows a list of common medications and how they may negatively affect the kidneys. This is not an exhaustive list and should be used in consultation with the provider or the nephrologist.
It is also important to remember that some medications commonly used for kidney patients can be harmful in certain situations. For example, a diuretic (water pill) can become dangerous if the patient is not eating or drinking well.
Courtesy: Lara Zakaria, PharmD CNS CDN IFMCP
Should the dose be adjusted to kidney function?
Many of the prescribed medications are excreted by the kidneys. Therefore, the doses of these medications should be adjusted according to the level of kidney function to avoid toxicity or side effects. Some medicines should be entirely discontinued at the advanced stage of kidney disease. This website can be accessed to see the dose adjustment needed for a specific drug according to the kidney function.
![]()
Does it interact with other medications?
Drugs can interact with each other in various ways. For example, a medication can affect the absorption of others by the gut. It may affect the way another drug is transported in the circulation. It may decrease or increase its breakdown by the liver or other organs. It can also affect its excretion by the kidneys or the gut. This interaction checker is a valuable tool for providers and patients to see if a drug that is being prescribed interacts with another one that the patient is already taking.
Does it affect micronutrients?
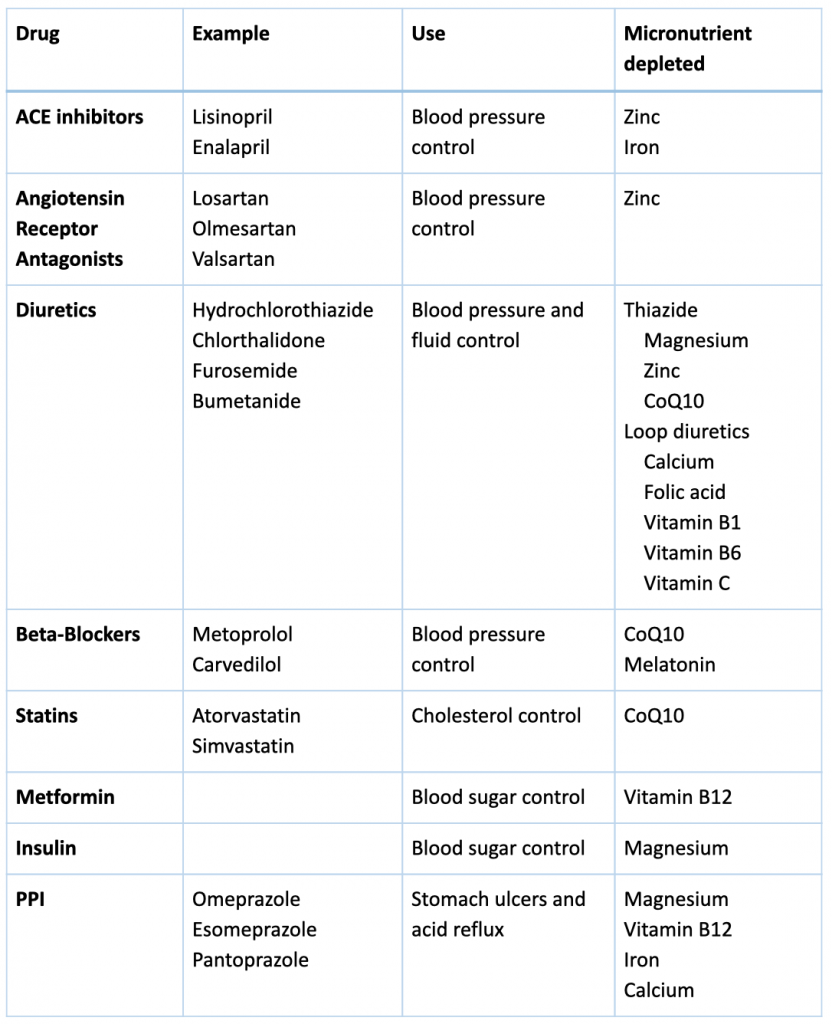
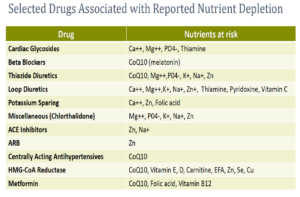
Micronutrients are essential for every structure and function in the human body, including but not limited to the function of the heart, blood vessels, and immune system. Thousands of enzymes in the body require micronutrients for optimal function. Some medications interact with micronutrients, and micronutrients may interfere with the action of drugs. The is a field of study called Drug-Induced Nutrient Depletion (DIND), and many books are written about it. The following table summarizes some of kidney patients’ most commonly used medications with their nutrient interactions.
The bottom line
Before taking a new medication, kidney patient should ask themselves and their provider the following questions: Is it necessary? Does it harm the kidneys? Does it interact with my other medications? Should the dose be adjusted for my kidney function? Does it interact with micronutrients? Please do not change or stop your medications without checking with your provider or nephrologist.
Download Your Copy!






The post Five questions kidney patients should ask before taking a new medication appeared first on Integrative Kidney.]]>
Metformin and CKD survey results
You can see the results of the survey in this earlier blog. It demonstrated that caution about the use of metformin in CKD is common among primary care physicians and other specialties. Nephrologists seem to be more comfortable with using it until the patient reaches stage 4 CKD. Most nephrologists, however, were not aware that metformin is associated with nutritional deficiencies. You can read the results of the survey in detail here.
What is metformin?
Metformin was first produced in 1922. However, since 1958 it has been used in the control of blood sugar in type 2 diabetes. It is a biguanide drug, a class of medications that inhibit the liver’s production of glucose, enhancing the body’s insulin sensitivity and lowering the amount of blood sugar that the intestines absorb. It is chemically developed from galegina, a natural guanidine compound found in Galega officinalis (French lilac, also known as goat’s rue).
In essence, metformin is an oral diabetes medication that helps control blood sugar levels. It is often used together with diet and exercise to improve blood sugar control in patients with type 2 diabetes mellitus. There are other off-label uses for metformin and it is currently being studied for the treatment of polycystic kidney disease.
Join us in the fight against kidney disease and receive the FREE Report “5 Pitfalls to Avoid When Caring for Kidney Patients”
Does metformin cause acute kidney injury?
For many years clinicians have been avoiding the use of metformin in kidney patients and specifically in those with diabetes. This is fueled by the FDA warning about the use of metformin in these patients due to concerns about lactic acidosis (discussed later). The original FDA warning was much more strict, but the more recent one issued in 2016 weighed in with more detail about metformin and kidney function. The new warning allows metformin to be used in patients who have worse kidney function. The newest warning indicates metformin can be used in patients who have an estimated glomerular filtration rate (eGFR) greater than 45 mL/min. Furthermore, metformin can continue to be used in existing patients whose eGFR remains over 30 mL/min.
As you saw from the survey, many primary care physicians and other specialists think that metformin can cause direct acute kidney injury. However, the literature shows that metformin can be protective in kidney disease. There is absolutely no evidence that metformin can lead to kidney injury. In fact, there is evidence to the contrary.
Download Your Copy!
Metformin clearance by the kidneys
Metformin does not undergo metabolism in the body, and it is eliminated unchanged in the urine. It is mainly cleared by tubular secretion in the kidneys. Metformin clearance is proportional to creatinine clearance. Therefore, although metformin can be used in patients with advanced kidney disease the dose of metformin should be decreased. The following table shows the recommended doses of metformin according to kidney function.
| Kidney function | Total daily metformin dose |
| Normal | 3000 mg |
| 45-59 ml/min | 2000 mg |
| 30-44 ml/min | 1000 mg |
| Less than 30 ml/min | Not recommended |
Metformin-induced diarrhea
The most common side effects of metformin are gastrointestinal. This is because one of the ways that metformin works is directly on the gut, altering glucose (sugar) absorption in the gut. Consequently, symptoms of nausea and diarrhea can occur especially in the first few weeks of taking it. That is why the patient should be started on a low dose to get used to it. Despite the statistic that 25% of patients taking metformin report diarrhea, only about 5% of those taking it had to stop it due to that side effect.
Metformin and lactic acidosis
The real reason why metformin was technically “banned” from use in CKD patients in previous years was due to the development of lactic acidosis. Lactic acidosis is a disease where lactic acid, a metabolic byproduct, accumulates in the blood. Lactic acid is mainly produced in small amounts by the muscles and red blood cells. It is formed when the body breaks down sugars to make energy under conditions of low oxygen (anaerobic glycolysis). This can occur during intense exercise or severe infection (called sepsis).
Metformin can induce lactic acidosis by shifting energy production in the cells toward anaerobic glycolysis. It also decreases the ability of the liver to consume lactic acid. Yet, in practice this is rare. In fact, it has been shown that lactic acidosis can occur in patients taking other oral blood-sugar-lowering medications at the same rate as metformin. Most case reports of metformin-induced lactic acidosis were in patients who have other conditions that lead to acute kidney injury (AKI) and lactic acidosis such as septic shock.
So, it is not that:

Instead, what happens is:

Finally, in a large retrospective study of patients with diabetes mellitus, metformin use was not significantly associated with lactic acidosis at kidney function levels higher than 30 ml/min/1.73 m2 (stage 3 or better).
Metformin and vitamin B12 deficiency
The association between long-term use of metformin and low vitamin B12 levels in type 2 diabetes mellitus patients is well-established. This is thought to be due to changes in the production of intrinsic factor in the stomach, which decreases vitamin B12 absorption in the intestine. Vitamin B12 deficiency is more pronounced if the patient is also taking a proton pump inhibitor such as omeprazole or histamine H2 receptor antagonist such as famotidine, which are medications used to treat acid reflux. Since diabetes can cause peripheral neuropathy, as well as vitamin B12 deficiency, can cause peripheral neuropathy, it can be confusing for diabetic patients on metformin and their practitioners.
Therefore, patients using metformin for a prolonged period should be screened initially and periodically for vitamin B12 deficiency. In addition, there is also growing evidence that other B vitamins, vitamin D, and magnesium can be impacted by metformin.
Bonus: Metformin’s impact on the gut microbiome
Because of metformin’s actions on the gut, it can also alter the intestinal microbiota for the better. Studies showed that metformin can enhance the growth of Akkermansia muciniphila, Butyrivibrio, Bifidobacterium, and Lactobacillus. In addition, it decreases the levels of some other bacteria like Intestinibacter. Metformin also promotes the production of the short-chain fatty acids that protect the intestinal barrier. In fact, some authors attribute some of metformin’s actions to its favorable impact on the gut microbiota and integrity.
The Bottom Line for Metformin and Kidney Disease
The answer to the question “Is metformin bad for the kidneys?” is generally no. Metformin can be used in patients with kidney disease. It actually leads to better outcomes in these patients. However, the risk of metformin-induced lactic acidosis increases in CKD stage 4 and above. It is, therefore, not recommended for use in these patients and patients with acute kidney injury. I also recommend avoiding it in patients with renovascular disease because their kidney function tends to fluctuate. Furthermore, metformin can be associated with vitamin B12 deficiency and patients should be screened initially and periodically for deficiency of this important vitamin.
The post To Metformin or Not To Metformin in CKD appeared first on Integrative Kidney.]]>While this is not official medical research, I aimed to identify current thoughts among nephrologists and primary care providers about its use in CKD patients. The survey results suggest that many practitioners avoid metformin in CKD based on outdated FDA guidelines. In fact, metformin has beneficial effects for kidney health and can safely be used in certain stages of CKD. In this blog, I will share the survey results. For the current evidence and recommendations for metformin use in kidney disease, read the second part of this blog, “To Metformin or Not to Metformin in CKD.”
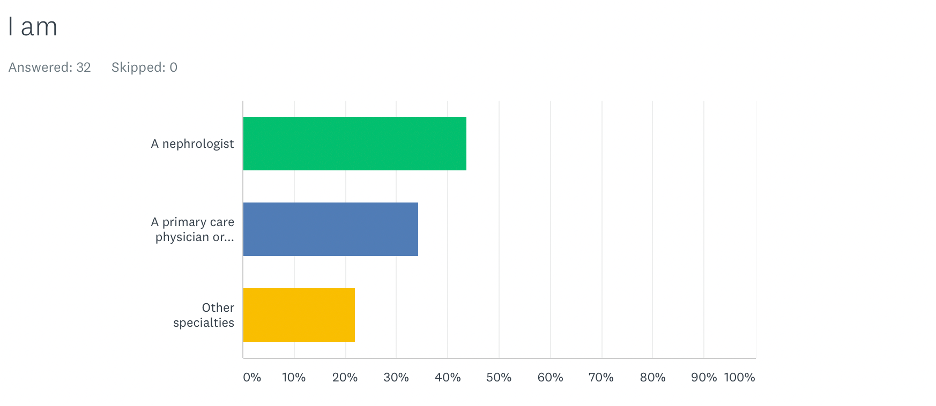
Participants in the Metformin and Kidney Disease Survey
We had 32 respondents: 44% of the respondents were nephrologists, 34% were primary care physicians, and 22% were from other specialties.
Join us in the fight against kidney disease and receive the FREE Report “5 Pitfalls to Avoid When Caring for Kidney Patients”
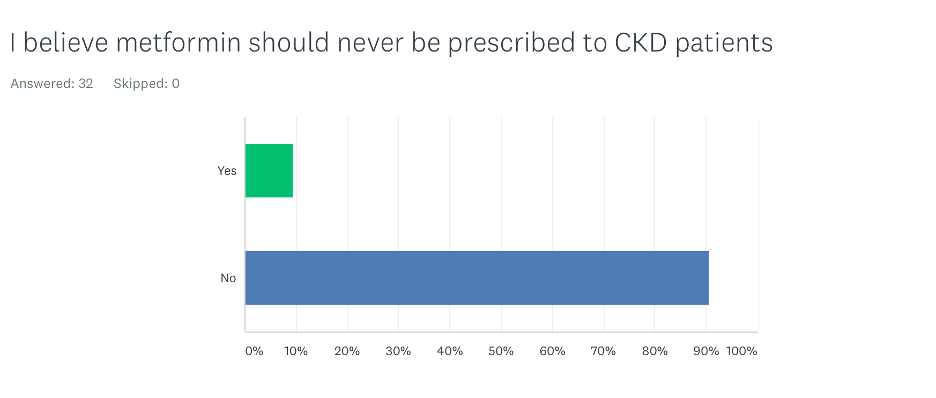
Should metformin be used in kidney disease patients?
Only 9% of participants thought that metformin should never be used in all CKD patients. All nephrologists believed that metformin can be used in patients with CKD. Among primary care providers, 27% believed that metformin should never be used in all CKD patients.
Does metformin cause acute kidney injury?
In the survey, 28% of participants believed that metformin causes acute kidney injury. The majority of those were primary care physicians. Only 7% of nephrologists believed that metformin causes acute kidney injury.
Block "fundamentals" not found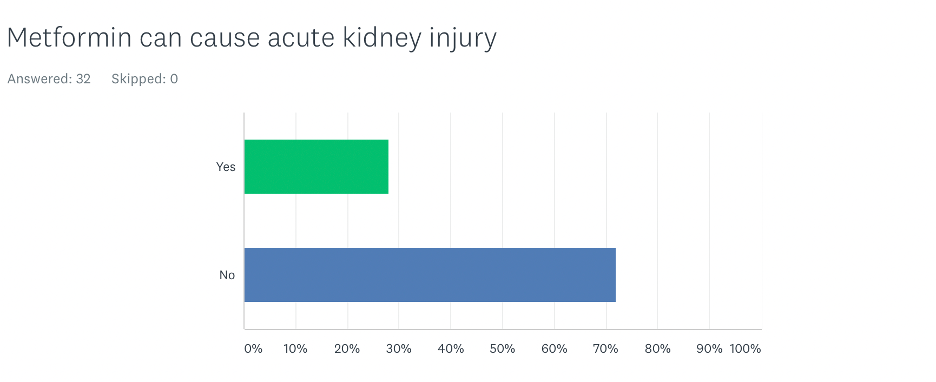
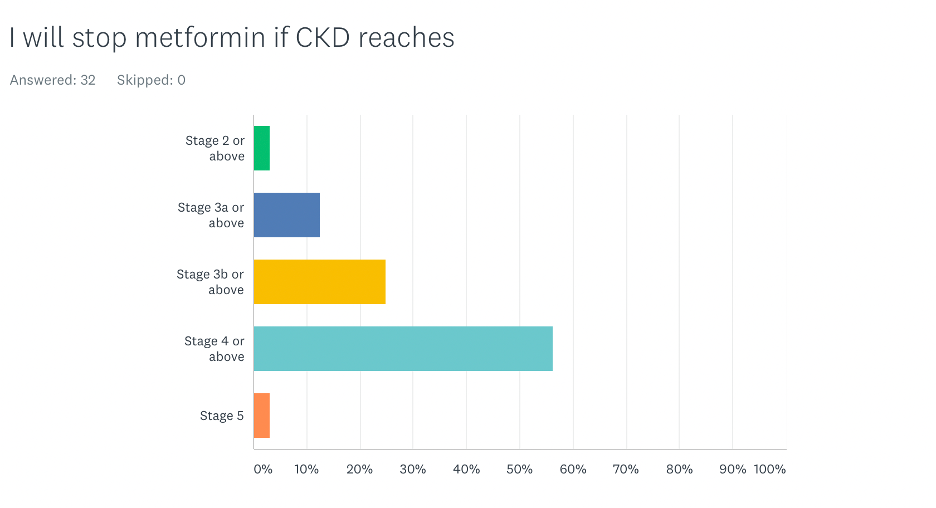
At what stage of CKD do you stop metformin?

The majority of participants (56%) believed that metformin should be discontinued when a patient reaches stage 4 CKD or above. Interestingly, 25% of the participants recommended discontinuing it if the patient reaches stage 3b CKD. Most nephrologists discontinued it when patients reached stage 4 CKD or above. Most physicians who discontinued it at earlier stages were primary care physicians.
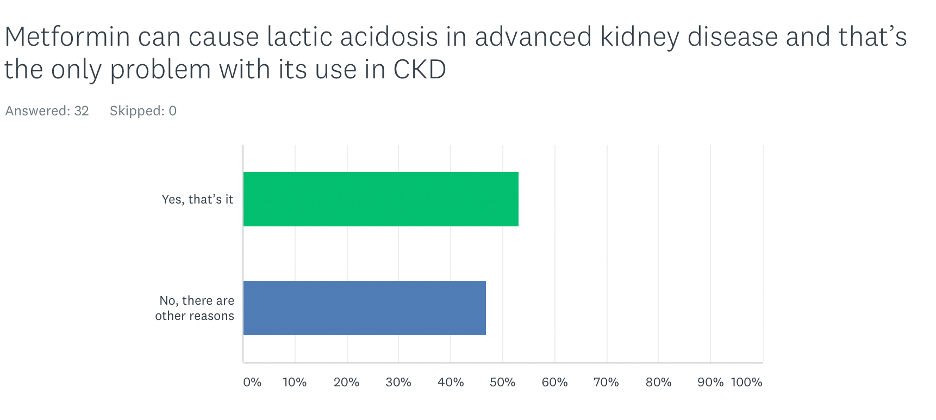
What is the problem with the use of metformin in advanced kidney disease?
This question may be suggestive, but about half of the participants believed that the risk of lactic acidosis is the only problem with the use of metformin in patients with advanced CKD. Interestingly, the majority of participants who believed there are other problems with the use of metformin in advanced kidney disease were non-nephrologists. One would think that nephrologists would be more aware of other risks beyond lactic acidosis.
When asked about specific reasons to avoid using metformin in advanced CKD, two rationales mainly emerged. Because metformin is removed from the body by way of the kidneys, one reason for its avoidance is the potential accumulation of excessively high levels of metformin in advanced kidney disease. The other reason was that metformin can be associated with diarrhea that can lead to volume depletion (loss of body fluids) and acute kidney injury.
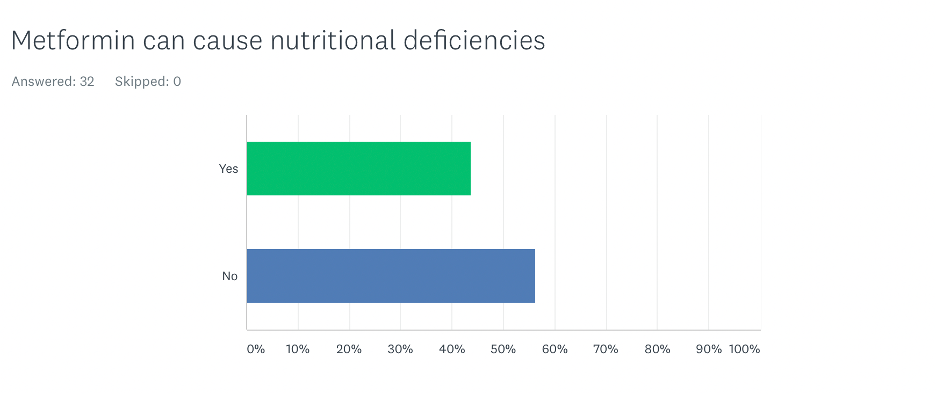
Can metformin cause vitamin B12 and other nutritional deficiencies?
Strikingly, 56% of participants were not aware of metformin and vitamin B12 deficiency or that it may cause depletion of other nutrients. Among nephrologists, this percentage was an amazing 79%.
The Bottom Line
Caution about the use of metformin in CKD is common among primary care physicians and other specialties. Nephrologists seem to be more comfortable with using it until the patient reaches stage 4 CKD. Most nephrologists, however, were not aware that metformin is associated with nutritional deficiencies. In the next blog, I will dig deeper into the research to find evidence-based answers to the questions presented in this survey.
Download Your Copy!

Angiotensin Converting Enzyme Inhibitors
Angiotensin Converting Enzyme Inhibitors (ACEi) are one of the main classes of blood pressure lowering medications in Kidney disease. ACEi (such as lisinopril) have been found in multiple studies to improve outcomes in diabetic and non-diabetic kidney diseases. However, it’s well documented that ACEi can lead to increased levels of potassium in the blood. This elevation may have many serious effects, especially on the heart and the muscles. Furthermore, supplementing with arginine, a precursor of nitric oxide sometimes used to support blood pressure, while taking an ACEi may further increase the risk of increased blood potassium levels.
The use of ACEi also induces zinc deficiency. By binding zinc, ACEi cause an increase in zinc excretion in the urine. Zinc Deficiency has many negative effects on the body, including cardiovascular and metabolic disease risk.
Angiotensin Receptor Antagonists
Another kidney medications and micronutrients interaction involves angiotensin receptor antagonists (ARBs). Just like ACEi, Angiotensin Receptor Antagonists (such as losartan) are one of the most commonly used blood pressure lowering medications in kidney disease. Like ACEi, ARBs also lead to an increase in potassium so electrolyte balance should be monitored closely. Also similarly to ACEi, evidence suggests that ARBs can also lead to zinc deficiency.
Using the powerful antioxidant alpha-lipoic acid (ALA), which can be used as a supplement, has been found to enhance the effects of ARBs by decreasing inflammation and oxidative stress that leads to cardiovascular risk from atherosclerosis.
Diuretics
Diuretics, also known as water pills, are used in kidney patients for blood pressure and fluid control. They are one of the major causes of kidney medications and micronutrients interactions. There are multiple classes of medications that fall into this broad category, and each affects minerals like potassium, magnesium, calcium and various vitamins differently.
For example, hydrochlorothiazide (HCTZ) and furosemide, can lead to potassium and magnesium deficiency so these nutrients are monitored very closely in patients prescribed these drugs. However, their effect on calcium varies. Thiazide diuretics (such as HCTZ) increase calcium retention while loop diuretics (such as furosemide) induce calcium depletion.
HCTZ can increase zinc loss in the urine leading to zinc deficiency. Furthermore, HCTZ can lead to CoQ10 deficiency (by inhibition of NADH oxidase) an antioxidant compound produced in our cells associated with reduced function of cardiovascular muscle and reduced skeletal muscle strength (more about CoQ10 below under statins).
Loop diuretics, including furosemide, have been found to induce deficiency of folate, vitamins B1, B6, and C . Furthermore, drug-induced calcium loss in the urine associated with this class of diuretics can lead to increased risk of bone loss and increased risk for kidney stones.
Beta-blockers
Beta-blockers (BB), such as metoprolol, are commonly used blood pressure reducing medications because they have been found to improve cardiac outcomes.
However, these medications exert their effect while inhibiting enzymes that are dependent on CoQ10 (including NADH-oxidase and succinoxidase). While these medications do not lead to CoQ10 deficiency per se, the concomitant presence of a CoQ10 deficiency for any other reason can lead to greater inhibition of the heart muscle efficiency as well as leading to worsening heart failure.
In addition, BB (especially metoprolol) have been found to decrease the production of melatonin, a compound naturally produced by the body that acts as an antioxidant and sleep inducer. The production of melatonin in the evening as part of our natural sleep-wake cycle induces sleep, and therefore depletion of melatonin causes sleep disturbances. Poor sleep is a major risk factor for progression of kidney disease, diabetes, and hypertension. In patients taking these medications, melatonin supplementation was found to improve sleep quality.
Statins (HMG-CoA Reductase Inhibitors)
Statins, including atorvastatin and simvastatin among many others, are the most commonly used class of cholesterol lowering medications. One of the major drug-induced nutrient depletions of statins is due to the inhibition of the formation CoQ10. Along with insufficient vitamin D blood levels, depletion of CoQ10 along with certain genetic factors is associated with an increased risk of developing a common side effect referred to rhabdomyolysis (muscle breakdown).
CoQ10 is produced throughout the body in the energy powerhouse of the cells. It is a major part of energy production and metabolic process. ”Co” stands for coenzyme, referencing its action in assisting enzymes in an energy production process called the electron transport chain (ETC). The ETC is an essential part of how energy is derived from carbohydrates and fat. Therefore, depletion of CoQ10 not only increases oxidative stress, but also has a significant effect on the function of every organ in our body, and particularly impact the cardiovascular and renal system. .
In addition,statins have been shown to deplete trace elements, including zinc, copper, and selenium. Furthermore, statins while lowering serum fatty acid concentrations (LDL, TG, etc), they also negatively alter the blood levels of important heart-protective polyunsaturated fatty acids (PUFAs while increasing inflammatory arachidonic acid levels. These drug-nutrient interactions are inconsistent from patient to patient, likely due to genetic variations, agent chosen, and dose. Therefore, monitoring lab and symptoms of deficiency or imbalance is ideal.
Metformin
Metformin is used to improve blood sugar by improving insulin sensitivity. Although some kidney patients might be taking metformin, it is not recommended for use in advanced kidney disease due to the increased risk of lactic acidosis.
Metformin is known to decrease the absorption of vitamin B12 by inhibiting the secretion of intrinsic factor, a compound needed to absorb B12 from food. B12 is a water-soluble vitamin and is essential for many processes, including energy production, production of endogenous proteins used for various cell functions including DNA repair, production of blood cells, myelin (cells that make up the nervous system), and some antioxidants. Therefore, supplementing vitamin B12 in patients taking metformin may prevent anemia, maintain brain health, cell production, and support the detoxification pathways.
Insulin
Insulin which is injected to lower blood sugar in diabetics can lead to significant loss of magnesium in the urine. Low magnesium can lead to significant effect on vascular, bone and heart health. In fact, supplementing magnesium in diabetics can improve insulin response.
Proton Pump Inhibitors (PPIs)
Proton Pump Inhibitors (PPIs) are one of the most commonly used drug classes globally, including in patients with kidney disease. Drugs belonging in this class include omeprazole and pantoprazole, which are commonly used for “acid reflux”, decrease stomach acid production leading to nutrient malabsorption and dysbiosis. They can lead to a decrease in calcium, iron, magnesium and vitamin B12. It’s also well-established that they also directly contribute to kidney injury. Despite that, their use remains common and we should remain vigilant in general.
Bottom Line
Many kidney medications can lead to micronutrient deficiencies with negative effect on outcomes and organ functions. The following table helps summarize these for you with general suggestions for supplementation. We recommend that you work with your integrative medicine provider to address complementary therapy to optimize you treatment and nutritional status.