Join us in the fight against kidney disease and receive the FREE Report “5 Pitfalls to Avoid When Caring for Kidney Patients”
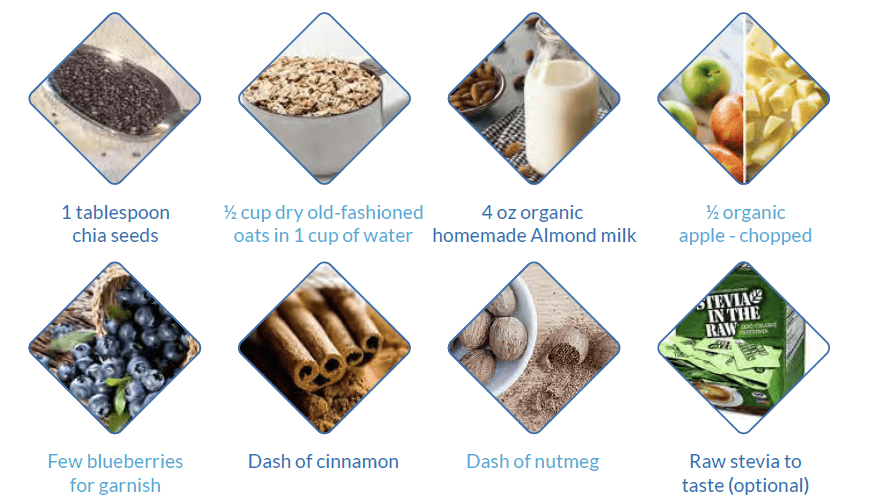
Breakfast Chia Apple Oatmeal
By Majd Isreb, MD, FACP, FASN, IFMCP
This is one of my favorite breakfast recipes. It is a healthy plant-based breakfast with 7 g protein and 10 g of fiber to start you day right.

Ingredients
Direction
- Boil 1 cup of water then add oats, chia seeds and chopped apple.
- Cook for 5 minutes, stirring over medium heat.
- Sprinkle cinnamon and nutmeg.
- Add raw stevia to taste
- Add 4 oz of almond milk if desired.
- Garnish with chopped apples and blueberries (optional)
Enjoy
Download Your Copy!






The post Breakfast Chia Apple Oatmeal appeared first on Integrative Kidney.]]>

Root Causes of Itching in Kidney Disease
Uremic toxin-induced neurologic changes
Several studies showed that patients with CKD have an imbalance of opioid receptors in the central and peripheral nervous system. Interestingly, itching in CKD correlates better with the level of uremic toxins than with glomerular filtration rate (GFR, a measurement of how well the kidneys are working). These toxins play an important role in these neurologic changes that are common in CKD. Most of these toxins are generated by the gut microbiome and are excreted by the renal tubules and not by glomerular filtration (or GFR). Measuring these toxins can be helpful. This can be done by a metabolomic test such as Genova’s Metabolomix+.
Download Your Copy!
Inflammation
CKD is an inflammatory disorder. Elevated inflammatory markers have been found to be associated with itching in kidney disease. Measuring inflammatory markers such as hsCRP, Th-1 cells, and IL-6 can be helpful in the assessment of the root cause of itching in CKD.
Dehydration
Dehydration can also lead to dry skin and worsens itching in CKD patients. Correcting the dehydration can be important in the management of itching.
Join us in the fight against kidney disease and receive the FREE Report “5 Pitfalls to Avoid When Caring for Kidney Patients”
Drug-induced itching
Many medications that are used in CKD have been associated with itching. These include calcium channel blockers, hydrochlorothiazide, and ACE inhibitors. In addition, other medications such as opioids, anticoagulants, and antibiotics can cause itching.
The itch-scratch-itch cycle
One of the major problems with itching is that it leads to scratching, and this can cause skin damage. The latter can cause further itching and the cycle continues.
Natural Treatments for itching in kidney disease
There are many steps you can take to get rid of itching in kidney disease and a kidney disease rash. The first step is to visit a healthcare provider to help you determine the root cause. You can download this two-page handout to guide you in the natural treatment of itching. There is hope that you’ll relieve this frustrating problem and have comfortable skin once again.
The post Root Causes of Itching in Kidney Disease appeared first on Integrative Kidney.]]>

Genetic testing for patients with kidney disease can have a remarkable impact on their care. The availability of “broad-panel genetic testing” for kidney patients ushers in a new era of nephrology and patient care. Tests that used to cost thousands of dollars and took months for results can now be done for a fraction of the cost in just a few weeks. New commercially available genetic tests utilize next-generation sequencing to identify multiple gene variants simultaneously. These tests can help in the management of kidney disease in multiple ways. In this blog, we will focus on the clinical utility of genetic testing for kidney transplant evaluation.
Genetic Testing for Kidney Transplant Evaluation
During the evaluation of a patient for a kidney transplant (the recipient), the assessment usually focuses on answering these questions:
- Can the recipient survive elective transplant surgery?
- Can the recipient tolerate immunosuppression after the transplant?
- Can the recipient have a good outcome?
In addition, evaluation of living donors try to answer questions about their suitability for donation and their risk of developing kidney failure in the future.
Living Donor Evaluation
One of the most pressing questions when evaluating a living donor is: Will this donor develop kidney disease in the future if s/he donates a kidney now? Several studies have shown an increased risk of the donor developing kidney disease after donation. This risk is higher if the donor and the recipient are related. This may indicate that genetic factors play a role in this risk.
In 2017, the Kidney Disease Improving Global Outcomes (KDIGO) Guidelines suggested that “transplant programs should have a strategy for evaluating for inherited kidney disease in donor candidates when there is a family history of kidney failure and the recipient’s cause of kidney failure is uncertain.”
These guidelines suggested genetic testing of living related donors with specific diseases such as focal segmental glomerulosclerosis (FSGS), atypical hemolytic uremic syndrome, Alport disease, sickle cell trait, and autosomal dominant tubulointerstitial kidney disease.
Genetic testing of a living relative donor can be especially important if the recipient has polycystic kidney disease. If this mutation is identified in the recipient, the donor can then be tested and excluded if s/he has the mutation. This can give greater assurance to both the donor and recipient.
Other genetic variants are associated with increased risk of chronic kidney disease (CKD) such as APOL1 gene variants that are associated with increased risk for nephropathy in patients of African ancestry. Incorporating testing for these genetic risk variants in the evaluation of the donor may help replace race for calculation of the so-called Kidney Donor Risk Index that is used to predict the longevity of the transplant graft.
While it is still too early to incorporate the genetic risk variants for diabetic kidney disease and IgA nephropathy in transplant evaluation, getting more clarity on the utility of the risk variants can have a tremendous impact on the care of current patients.
Recipient Evaluation
Kidney disease is silent in its progression and symptoms do not develop until the advanced stages of CKD. One in 10 patients with advanced kidney diseases presents with end-stage kidney disease (ESKD). In many of these cases, the laboratory workup is inconclusive, and their kidneys are often too atrophic to biopsy. Unlike kidney biopsies, genetic data can be informative even after ESKD has developed.
Genetic evaluation of the recipient is, therefore, helpful in identifying the causative mutation that could have led to the disease. Using targeted gene testing, researchers were able to identify pathogenic mutations in 19% of waitlisted transplant patients under the age of 40. Broad panel genetic testing can likely have an even higher yield. Indeed, broad panel genetic testing has been shown to identify the cause of CKD in up to one-third of the patients with an unknown cause.
Genetic testing of the recipient can also help in providing individualized post-transplant care. Finding a specific mutation that leads to a localized disease in the kidneys can decrease concerns about the recurrence of the disease after transplantation.
Also, a genetic diagnosis can often point to the likelihood of disease in another organ and can prompt referral and evaluation.
Currently, researchers are collecting phenotypic and genetic information on patients receiving transplants in the iGeneTRAiN consortium. Analyzing this data in the future may have a significant impact on our understanding of transplant graft outcome.
Pharmacogenomics
Wouldn’t it be a relief to be able to predict in advance how someone might respond to a medication? This would save time, eliminate guesswork, and improve patient outcomes. Thanks to advances in a field of genetics called pharmacogenomics (PGx), clinicians have begun to use genetic information to personalize drug therapy.
Accurate pharmacogenomics data are now available on two transplant medications: tacrolimus and azathioprine. Although the latter is not commonly used, the former is used often. Tacrolimus is metabolized by the enzyme encoded in the gene CYP3A5. Variants in this gene can classify the patient into one of three phenotypes: extensive metabolizer, intermediate metabolizer, and poor metabolizer. Indeed, pharmacogenomic data can now be used to optimize the initial dose of tacrolimus.
Many other medications commonly used by patients have pharmacogenomic data which can also be used to optimize their dosing. Medications such as clopidogrel, voriconazole, and allopurinol are a few of these. We discussed these medications in-depth in our previous blog about pharmacogenomics.
The Bottom Line
Genetic testing is gradually becoming a significant part of the transplant evaluation of the donor and the recipient. It is particularly useful in the evaluation of living donors with a family history of kidney disease. This data has the potential to transform the care of kidney transplant patients and improve their outcomes.
The post Clinical Utility of Genetic Testing for Kidney Transplant Evaluation appeared first on Integrative Kidney.]]>
Current evidence suggests that genetics play a role in the development of kidney disease. Common genetic disorders associated with kidney disease include polycystic kidney disease, Alport’s Syndrome and Fabry’s disease. The advances of genome-wide association studies (GWAS) helped identify several hundred other genes linked to kidney diseases. This made genetic testing a useful tool in the management of kidney disease patients. In this blog, we will detail the benefits of broad-panel genetic testing in kidney disease management.
Next Generation Sequencing
Various methods for identifying genetic variants have been used in the past. The exome is that 2% of the genome that codes for all biological proteins. Next generation sequencing is a new technology that allows DNA sequencing of the entire human exome within a single day. It also captures a broader spectrum of variations that can affect the genetic code. This revolutionary technology can identify mutations associated with CKD. It can also recognize variants associated with an increase in risk or severity of CKD. It is now available for kidney disease patients. This type of “broad-panel genetic testing” can transform care for patients with kidney disease.
Clinical benefits of genetic testing in kidney disease management
Identify diagnosis of unknown causes
While diabetic and hypertensive kidney diseases are the most common causes of kidney failure, there are others. There are instances when providers find themselves unable to identify the cause of kidney disease. Indeed, in some cases, urinalysis is actually “bland” and the workup to identify the cause of kidney disease is negative.
Even a kidney biopsy may not be helpful. It may show glomerulosclerosis and fibrosis (scarring). This does not help identify the original cause of kidney disease. Genetic testing can have a tremendous value in these cases. In fact, whole exome sequencing was able to diagnose up to one third of the patients who had unknown causes of kidney disease.
Reclassify a clinical diagnosis
It is common for providers to label kidney disease patients with unknown causes as hypertensive kidney disease or “nephrosclerosis”. This is because hypertension is common in kidney disease patients. Studies have shown that 60-90% of patients with chronic kidney diseases have high blood pressure. It is often not clear which came first, hypertension or kidney disease. It is possible that patients who were diagnosed with hypertensive kidney disease have another cause. In fact, studies have shown that up to a quarter of kidney diseases can be reclassified with a broad-panel genetic testing.
Target the therapy and workup
Broad-panel genetic testing can help providers avoid unnecessary procedures, tests, and treatments. It gives accurate and “molecular level diagnosis”. It provides a better idea of the outcome of the specific kidney disease. It also helps providers avoid the use of immunosuppressive medications in patients with genetic causes of kidney disease. Furthermore, it can guide therapy for specific genetic causes that we currently have treatment for such as Fabry’s disease. This type of testing may, indeed, eliminate the need for a kidney biopsy.
Role in kidney transplant
Genetic testing can have a tremendous impact in guiding kidney transplant and in the care of kidney transplant recipients. Kidney transplant donors can be pre-screened by broad panel genetic testing to assess if they carry any genetic kidney disease risk. While carrying the genes does not necessarily indicate that the donor will have the disease, it can play an important role in selection. This is especially true for living donor kidney transplant when the recipient has a known genetic kidney disease, and the donor is too young to have any manifestations.
In addition, many immunosuppressive medications that are used by kidney transplant patients are metabolized by well-established pathways that can be affected by genetic SNPs.
Having this genetic information can help providers prescribe the proper dose of immunosuppressive medications which is critical in transplant patients to avoid rejection or toxicity. This evolving field is called pharmacogenomics.
Help with management of kidney patients
Broad panel genetic testing can identify patients who are at risk for kidney disease, reclassify the exact cause of kidney disease, and guide treatment. Knowing the molecular basis of some kidney diseases can guide lifestyle modification interventions, future development of drugs, and gene therapy. It can also identify early complications outside the kidneys that can be related to the specific genetic disease and prompt early interventions.
Available broad panel genetic tests
Broad panel genetic tests are now available for providers and patients, and are relatively inexpensive. Many of them are covered by insurance companies. We have utilized Natera’s Renasight broad panel genetic test for this purpose. It provides next generation sequencing for 382 genes that are associated with kidney disease. There are also other genetic testing companies that test a small panel of genes for free to identify patients for drug or gene therapy.
The Bottom Line
We are at the dawn of a new era in nephrology and kidney care. Broad panel genetic testing will revolutionize kidney disease management. Our genes are not our destiny, but we cannot change our destiny without knowing our genes.
The post Genetic testing in kidney disease appeared first on Integrative Kidney.]]>
The basics
As you may remember, each person inherits 46 chromosomes, 23 from each parent. These chromosomes house the genetic code that determine the characteristics of each person. They are composed of DNA which is a long and windy spiral made up of millions of nucleotides. There are 4 nucleotide bases (adenine, cytosine, guanine, thymine), the sequence of which determines how genetic traits are expressed.
This nucleotide sequence forms the foundation of about 22,000 genes. Our cells read the genetic sequence and use it to make thousands of proteins which are essential for carrying out biological functions that maintain life. In other words, you can think of the cells as protein factories. The DNA code provides the blueprint for all the workers to create proteins. These proteins can function as enzymes, receptors, or other structures that are important for sustaining life.
Errors in the code
Alterations in the sequence of nucleotide bases cause errors in the code and affect the efficiency of the protein production process. These may sometimes lead to disease or increased risk for disease. Interestingly, on occasion they may have no effect on risk and may even be protective against disease. There are three major changes that can occur in the code:
- Single-nucleotide substitution: this is also called single-nucleotide polymorphism or SNPs. These are common.
- Insertion or deletions (indels): a small stretch of DNA can be inserted or deleted from the code.
- Structural variation: a large-scale change or rearrangement in the DNA.
It is fascinating that a single variation in one nucleotide among the set of 3 billion in our DNA can sometimes cause a severe and deadly disease and other times have no effect whatsoever.
Why genetics are important?
Genetics play an essential role in many functions in the human body. Genetic changes can affect the type of food that a person prefers to eat. For example, genetic variants in bitter taste receptors in the tongue have been associated with decreased intake of vegetables and increased obesity. Genetic changes can also affect digestion, and absorption of food. They can modify the way we metabolize drugs, and toxins. They can alter the function of vitamins and other nutrients and their interactions.
The genetics of disease risk
For a long time, scientists have been trying to study how variations in genes lead to diseases. Past efforts focused on identifying inherited diseases in the so-called Mendelian patterns. However, recent advances in GWAS studies are making it more possible to identify genetic changes that can be associated with increased risk of a disease. Genetic variations in one or several genes can lead to minor changes that collectively may increase the susceptibility for certain common diseases such as diabetes and high blood pressure. This is an evolving field of study and we will continue to learn about it every day.
Genetics of kidney disease
There are well known and relatively common genetic disorders such polycystic kidney disease, Alport’s Syndrome and Fabry’s disease. GWAS studies has identified more than 500 genes that are associated with kidney diseases. Current evidence suggests that a significant genetic component plays a role in the development of kidney disease. These are evident from the ethnic variabilities in certain diseases such as the higher incidence of IgA nephropathy among Asians.
Genetics can also determine the severity of a kidney disease, the age of onset and the likelihood of ending up with End-Stage Kidney Disease. For example, different gene mutations that can cause polycystic kidney disease can have different outcomes.
In addition, genetic variations can explain the differences in susceptibility of the kidneys to systemic disease such as diabetes and lupus. These variations may explain why some people with diabetes get severe kidney disease while others don’t.
Finally, alterations in several genes have been associated with increased risk for CKD. There are several candidate genes. Mutations in the UMOD that encodes uromodulin is one of these candidates. Uromodulin, which used to be called Tamm-Horsfall protein, is excreted in certain portions of tubules and protects from urinary tract infections. The Shroom3 gene is another candidate that has been associated with increased risk for CKD.
Next generation sequencing
Various methods for identifying genetic variants have been used in the past. Next generation sequencing is a state-of-the-art technology that allows DNA sequencing of the entire human genome within a single day. It also captures a broader spectrum of variations that can affect the genetic code. This revolutionary technology is now available for kidney disease patients and can identify various mutations that are associated with CKD or can increase the risk or severity of CKD.
The Bottom Line
Genetics are one of the factors that lead to the development of kidney disease. For genes and their variants to contribute to a disease, we need to understand all of the factors that explain why people with the same variant may have different outcomes. Understanding the interaction between genetics, epigenetics and environment are crucial in this regard. Ongoing research in this field will not only increase our understanding of kidney disease risk but our ability to find various lifestyle modifications and therapies that can help decrease the burden of CKD worldwide.
Professionals: You can get free CME and learn more about genetics of kidney disease here.
The post Genetics of Chronic Kidney Disease appeared first on Integrative Kidney.]]>