Join us in the fight against kidney disease and receive the FREE Report “5 Pitfalls to Avoid When Caring for Kidney Patients”
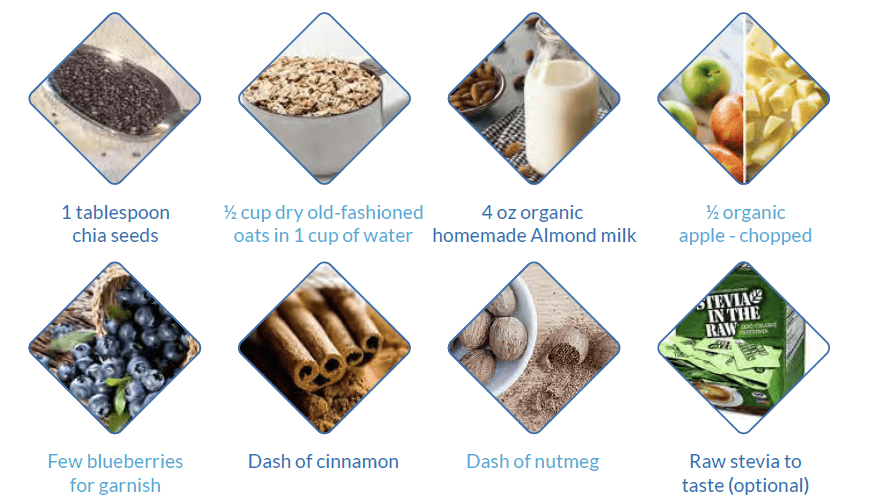
Breakfast Chia Apple Oatmeal
By Majd Isreb, MD, FACP, FASN, IFMCP
This is one of my favorite breakfast recipes. It is a healthy plant-based breakfast with 7 g protein and 10 g of fiber to start you day right.

Ingredients
Direction
- Boil 1 cup of water then add oats, chia seeds and chopped apple.
- Cook for 5 minutes, stirring over medium heat.
- Sprinkle cinnamon and nutmeg.
- Add raw stevia to taste
- Add 4 oz of almond milk if desired.
- Garnish with chopped apples and blueberries (optional)
Enjoy
Download Your Copy!






The post Breakfast Chia Apple Oatmeal appeared first on Integrative Kidney.]]>

The root cause of IgA nephropathy
IgA nephropathy is a kidney disease that is defined by the pathologic appearance of glomerular deposition of IgA immune complexes. However, this definition does not address the root cause of the disease.
It has been increasingly recognized that IgA immune complex that deposit in the kidneys predominantly contain polymeric IgA1 lacking galactose within its O-glycosylated hinge region.
In this study, researchers found that patients with IgA nephropathy have elevated levels of certain B cells that are enriched for λ light chains. These cells are predestined for homing to upper respiratory and digestive tract mucosal tissues. In the mucosal tissues, these B cells mature and excrete abnormal IgA in the setting of upper respiratory or digestive infection. You can read more IgA nephropathy by reading our blog here.
Join us in the fight against kidney disease and receive the FREE Report “5 Pitfalls to Avoid When Caring for Kidney Patients”
Metformin: Some people love it and some people hate it… But it sure is getting a lot of attention lately
This study was done in rats with “non-diabetic kidney disease.” CKD was established in these rats by feeding them high adenine diet. Then they were randomized to receive either metformin or canagliflozin (an SGLT-2 inhibitor).
Metformin, but not canagliflozin, halted the decline in kidney function. Additionally, kidneys of metformin-treated animals showed less interstitial area and inflammation as compared to the vehicle group.
Metformin is increasingly being studied in humans for various kidney diseases. If used judiciously it may be a cheap alternative to preserving kidney function.
Download Your Copy!
Tremor + gum disease + nephrotic Syndrome = ?
In this study, investigators in Beijing looked into the manifestation of mercury poisoning in 172 patients. 26.74% of these patients had kidney injury (3/4 were women) and most of them had nephrotic syndrome. The most common finding on the biopsy was membranous nephropathy.
Other findings of chronic mercury poisoning were neurotoxicity and gingivitis. Chelation with DMPS alone was as effective as chelation and prednisone in reversing kidney injury.
The most common source of exposure without kidney disease was industrial exposure. Interestingly, the most common source of exposure leading to kidney disease was cosmetics containing ionic mercury (mercury concentration in one of the patients cosmetic was 4600 mg/kg – national standards are < 1 mg/kg).
Join here to receive FREE monthly updates on the latest research in Integrative Nephrology straight to your inbox.
We would love to here your feedback. Let us know what you think of these educational materials and if you like us to focus on certain topics. Email us at info@inkidney.com
The post April Research And News appeared first on Integrative Kidney.]]>

Cold exposure
Cold exposure, such as cold showers, has many benefits for kidney patients. It increases endorphins and fights off depression. It improves metabolism and circulation. Most importantly, it stimulates the vagus nerve and improves renal circulation. It may also soothe itchy skin which is common in CKD patients. In addition, cold showers help with post-workout muscle soreness.
The benefits of a cold shower begin when the water temperature dips to 60 degrees Fahrenheit. This is 40 degrees lower than the typical steamy shower. To take a cold shower, start with your usual hot shower, then turn the knob to cold at the end of your shower. Lower the temperature gradually at the end of your shower every day. The benefits start with thirty seconds under the cold water. Maximum benefits are reached in three minutes.
Join us in the fight against kidney disease and receive the FREE Report “5 Pitfalls to Avoid When Caring for Kidney Patients”
Vagus nerve breathing exercises
Deep and slow breathing can activate the parasympathetic system. In fact, deep breathing is one of the best ways to lower stress in the body. It sends messages to the brain to calm down and relax by activating the vagus nerve which helps lower heart rate and blood pressure. There are various ways to perform deep breathing. Here, I will discuss the 4-7-8 breathing technique.
This technique uses belly breathing. It can be performed sitting or lying down as follows:
- Start by putting one hand on the belly and the other one on the chest.
- Take a deep slow breath from the belly while silently counting to 4. The chest should not move.
- Hold the breath while silently counting to 7.
- Breathe out completely while silently counting to 8.
- The process can be repeated 5 to 10 times until feeling relaxed.
Singing, humming, chanting, and gargling
These activities have also been shown to improve heart rate variability and can also activate the vagus nerve because it is connected to the vocal cords. These benefits can be achieved by 10 minutes of singing, humming, chanting, or gargling every day.
Probiotics
The fact that probiotics have been found to support stimulation of the vagus nerve is another piece of evidence for the importance of the gut-brain axis. Healthy microbiota produce short-chain fatty acids, such as butyric acid, which can activate the vagus nerve and send messages from the gut to the brain. It is highly beneficial to get most probiotics through diet. However, if supplements are used, it is recommended to use good quality broad-spectrum probiotics.
Download Your Copy!
Meditation
Meditation has been found to increase vagal tone and positive emotions. Meditation for 10-15 minutes is a great way to start the day, manage stress, and stimulate the vagus nerve. There are many ways to meditate and many types of meditations. Mindfulness meditation is the most tested in kidney patients. It has been demonstrated to improve the quality of life, reduce anxiety and depression, reduce sympathetic overactivity,improve sleep, and improve blood pressure.
To practice mindfulness meditation such as Benson’s relaxation technique, follow these steps:
- Sit in a comfortable position or on a meditation cushion.
- Close your eyes.
- Relax your shoulders and muscles.
- Focus on breathing.
- Say a word with every exhalation. A positive word like “gratitude” can be used. As the mind starts racing, which distracts from the breath, the person returns to the word.
Practicing this every day will improve the experience and compound the benefits with consistency.
Omega-3 fatty acids
Among the many benefits of omega-3 fatty acids are increased vagal activity. The best way to reap the benefits of omega-3 fatty acids is by eating fatty fish twice per week, but if that is not an option due to protein restrictions or dietary choices, supplementation is an option. Other food sources include nuts and seeds such as walnuts and flaxseed. It is important that the supplement contains enough eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), which are the most powerful omega-3 fatty acids. The dose is at least 500-1,000 mg of EPA-DHA three times a day.
Exercise
One of the best vagal tone exercises is exercise itself. Exercise is linked to better mental health and stimulation of the vagus nerve. It may be one of the most underutilized yet effective interventions for the prevention and treatment of kidney disease. It has been shown to reduce the risk of CKD, help with blood pressure and glucose control, and improve health-related quality of life. Exercise also induces a positive influence on mental health, mood, and stress levels by stimulating the vagus nerve.
The best type of exercise is the one that you do. What I mean by that is don’t get discouraged by trying to find the perfect type of exercise and do anything that works best for you. Having said that, studies on exercise in CKD have included resistance training and aerobic activities that use large muscle groups continuously such as walking, cycling, and jogging.
High-intensity interval training (HIIT) offers superior benefits in individuals with metabolic diseases such as diabetic kidney disease. Studies of HIIT in CKD have shown that it is a safe and feasible option for individuals with CKD.
Those who are new to exercising should start slowly and gradually get to 20-30 minutes of strenuous exercises 5-6 days a week. It is best to alternate between aerobic exercises and resistance training. For those who are 50 years of age or older, it is important to check with your provider before engaging in strenuous exercises.
Massage therapy
Massage therapy has also been found to be associated with improved vagal tone. The stimulation of pressure receptors leads to an increased vagal activity which, in turn, seems to mediate the diverse benefits of massage therapy. Functional magnetic resonance imaging data suggested that moderate pressure massage was represented in the part of the brain involved in stress and emotion regulation.
Socializing and laughing
Finally, increased social connection and laughing have been linked to increased positive emotions. Increased
positive emotions, in turn, produced increases in vagal tone, which puts the body in a rest and repair state.
The bottom line
Stimulating the vagus nerve can turn on the parasympathetic nervous system, improve renal blood flow, and modulate inflammation in CKD. Improve kidney health using these natural techniques to turn on the vagus nerve and turn off stress: a cold shower, breathing exercises or meditation, singing or humming, probiotics, omega-3 fatty acids, exercise, massage, and social connection. Check out my 1-hour morning routine for kidney health that incorporates many of these techniques.
The post Nine Ways to Naturally Stimulate the Vagus Nerve, Lower Stress, and Promote Kidney Health appeared first on Integrative Kidney.]]>
3 years of lifestyle interventions improved exercise capacity and decreased the losses in neuromuscular and cardiorespiratory fitness in CKD patients
In this study, researchers randomized 161 patients with stage 3-4 CKD to either get usual care or usual care plus lifestyle “intervention” for 3 years.
The lifestyle intervention comprised of care from a multidisciplinary team, including a nephrologist, nurse practitioner, exercise physiologist, dietitian, diabetes educator, psychologist, and social worker.
The patients were coached for 8 weeks and then followed for 34 months with a home-based program.
The study did not look at the progression of CKD but it found that a 3-year lifestyle intervention doubled the percentage of CKD patients meeting physical activity guidelines, improved exercise capacity, and decreased the losses in neuromuscular and cardiorespiratory fitness.
It appears that the study mainly focused on exercise. So imagine the benefit of a comprehensive lifestyle modification plan that includes nutrition, exercise, stress management, sleep improvement, and attention to toxin exposure and gut-kidney connection. That’s what we focus on.
Join us in the fight against kidney disease and receive the FREE Report “5 Pitfalls to Avoid When Caring for Kidney Patients”
Curcumin powder did not improve markers of vascular dysfunction in PKD
This is essentially a negative study.
It demonstrated that Curcumin powder did not improve markers of vascular dysfunction in children and young adults with PKD. The study was conducted for only one year using a dose of 25 mg/kg per day of curcumin.
This is a classic supplement or nutrient study that is usually underpowered or conducted for short periods of time for a disease that takes years or even decades to evolve. Nevertheless, the study proved that short-term use of curcumin is not beneficial for vascular health for young patients with polycystic kidney disease.
Low serum zinc levels were associated with infections in CKD patients
This did not really need research but it is now studied and it is official: Low zinc levels in patients with CKD lead to infection (..well among other things).
This retrospective study analyzed data from 299 CKD patients who had serum zinc levels checked to evaluate anemia. They used the level of 50 mcg/dl as the cutoff between low or “high” zinc values.
Low serum zinc values remained an independent risk factor for infection-related hospitalization. This was especially true for patients taking proton pump inhibitors (PPIs) medications.
Read about the effect of Zinc on kidney health in this blog.
Download Your Copy!
Join here to receive FREE monthly update on the latest research in Integrative Nephrology straight to your inbox.
We would love to here your feedback. Let us know what you think of these educational materials and if you like us to focus on certain topics. Email us at info@inkidney.com
The post January Research and News appeared first on Integrative Kidney.]]>Low magnesium levels have been associated with a number of adverse events, such as high risk for heart disease. However, little is understood about magnesium and kidney health. Here, we will discuss the potential benefits of magnesium on the kidneys. This is one of two articles on magnesium and kidneys. For more on how to test and treat kidney patients with magnesium deficiency, see part two, “Magnesium Deficiency: Assessment and Management for Better Kidney Health.”

Dietary sources of magnesium
A daily intake of 3.6 mg/kg is necessary to maintain magnesium balance in humans under normal conditions. This is estimated to be between 320 to 420 mg/day (13–17 mmol/day) for adults. Sadly, there has been a steady decline in magnesium content in cultivated fruits and vegetables over the past 100 years. This is due to depletion of magnesium in soil over time. This, along with the rise of ultra-processed food, sodas, and taking medications such as proton pump inhibitors and diuretics that deplete magnesium levels (polypharmacy), has led to rising prevalence of magnesium deficiency.
Traditionally, the highest food sources of magnesium are:
- Leafy greens (78 mg/serving on average)
- Nuts (80 mg/serving on average)
- Pumpkin seeds have the highest level of magnesium per serving (156 mg).
- Whole grains (46 mg/serving on average)
A complete list of foods high in magnesium can be found here.
Can Magnesium Help Kidney Function?
There are many potential benefits of magnesium for kidney health including improving blood pressure control, insulin sensitivity, bone health, vascular health, and preventing kidney stones. Let’s explore the data.
Magnesium and blood pressure control
Magnesium supplementation may help reduce blood pressure (BP) by increasing the production of nitric oxide. Nitric oxide acts as a signaling molecule that helps relax blood vessels, which lowers BP. In fact, a review of 34 studies showed that supplementing magnesium with an average dose of 368 mg per day for 3 months can decrease systolic BP by 2.00 mmHg and diastolic BP by 1.78 mmHg. This supplementation was accompanied by 0.05 mmol/L increase in serum magnesium levels.
Download Your Copy!
Magnesium and insulin sensitivity
Diabetes is one of the major risk factors for kidney disease worldwide. Higher dietary intake of magnesium has been correlated with lower diabetes incidence. A review of 18 studies in people with diabetes showed that magnesium supplements reduced fasting plasma glucose levels. In people who are at high risk for diabetes, magnesium supplementation significantly improved plasma glucose levels after a 2-hour oral glucose tolerance test. These effects are thought to be due to the effects of magnesium on insulin receptors and signaling that allows for improvement in glucose transport and utilization.
Magnesium and vascular health
Magnesium levels have been associated with a lower incidence of cardiovascular disease. In fact, supplementing with magnesium was associated with improvement in vascular flow and endothelial function. Endothelial function refers to the lining of the blood vessels, which is involved in regulating blood vessel health and blood clotting.
Studies in patients receiving dialysis have shown that having a lower serum magnesium level is a significant risk for cardiovascular mortality. Laboratory data show that magnesium inhibits high phosphate-induced calcification of vascular smooth muscle cells. Calcification of arteries is a strong predictor of heart disease and heart-disease-related death.
Magnesium and vitamin D
Magnesium is essential to vitamin D metabolism. Vitamin D that we eat or make in our skin from sun exposure circulates in the blood and is bound to vitamin D binding protein (VDBP). VDBP binding activity depends on adequate magnesium levels. In addition, magnesium is an essential cofactor for the enzymes that activate vitamin D. Studies have demonstrated that magnesium deficiency is associated with impaired vitamin D metabolism.
On the other hand, taking large doses of vitamin D can induce severe depletion of magnesium. This is thought to be due to the overutilization of magnesium. Therefore, adequate magnesium supplementation should be an important part of vitamin D therapy.
Adequate magnesium supplementation should be an important part of vitamin D therapy.
Share on X
Magnesium and bone health
Besides magnesium’s effects on vitamin D metabolism, it is an essential component of hydroxyapatite, an essential component of bone and teeth. In fact, 60% of total Mg is stored in the bone. Low magnesium intake was found to be associated with lower bone mineral density in postmenopausal women. Magnesium deficiency contributes to osteoporosis directly by acting on crystal formation and on bone cells and indirectly by impacting the secretion and the activity of parathyroid hormone (PTH) and by promoting oxidative stress and inflammation.
In addition, a review of 8 studies looked at magnesium and chronic kidney disease (CKD). The study investigated magnesium supplementation on parameters of CKD-related mineral bone disease (CKD-MBD). Mg supplementation improved PTH levels and carotid intima-media thickness (CIMT). Low serum Mg levels were also found to impact PTH and worsen osteoporosis in CKD patients, particularly with diabetes.
Magnesium and kidney stones
Mg acts as an inhibitor of calcium oxalate crystallization and stone formation in the urine. It also decreases the absorption of dietary oxalate in the gut. Mg supplementation in patients with kidney stones was found to decrease the incidence of stone formation even in patients without signs of Mg deficiency.
Magnesium as a phosphate binder
Hyperphosphatemia (high phosphate level) is common in advanced kidney disease. Many kidney patients with stage 4 and above use binders that bind phosphate (or “phosphorus,” as it is commonly known) in the food and prevent it from getting absorbed. High phosphate levels have been associated with poor bone and vascular health in kidney patients. In fact, higher dietary phosphate load can be seen in earlier stages of CKD, and it can do harm even before it is detected.
Magnesium carbonate has been successfully used as a phosphate binder. Magnesium based phosphate binders were also found to reduce vascular calcifications in rats with kidney disease. Iron-magnesium hydroxycarbonate was also studied and found to be well tolerated and can effectively lower phosphate levels in dialysis patients. It is essential to know that most of the magnesium used as a phosphorus binder will not be absorbed.
The bottom line on magnesium and kidneys
Magnesium is essential to many biological functions. It has many health benefits for kidney, bone, and vascular health. Optimizing magnesium status is, therefore, an important step in the integrative approach to kidney health. In part two of this blog, “Magnesium Deficiency: Assessment and Management for Better Kidney Health,” we will discuss practical steps for figuring out a person’s actual magnesium status, the best form of magnesium to take, and the dose I recommend for each condition.
The post Magnesium and kidneys appeared first on Integrative Kidney.]]>We combed through multiple medical journals looking for the latest research on the Integrative approach to kidney health. We know your time is valuable so we curated and summarized these studies for you. Welcome to the November edition of InKidney Research and News.

Is phosphorus toxic to the kidneys?
In this detailed study, researchers found that excessive intake of phosphate (phosphorus) increases a substance called FGF-23. One of FGF-23 main tasks is to maintain phosphorus balance in the blood. It does that by increasing the excretion of phosphorus in the urine. This study found that the presence of high phosphorus in the kidney tubules causes them to bind with calcium forming tiny crystals that are very toxic to the tubular cells and leads to fibrosis. Investigators found that a level of FGF-23 above 53 pg/mL is associated with progression of kidney disease in humans.
Coffee and caffeine consumption and the risk of kidney stones
Investigators used Mendelian randomization to study the link between coffee consumption and the risk of kidney stones. They looked into the UK and Finland genetic databases and tried to find the association between coffee drinking genotype and kidney stone phenotype.
The study found that genetically predicted coffee and caffeine consumption was associated with a lower risk of kidney stones. This supports other observational studies that indicated the same.
But of course, the study means that consumption of black coffee is associated with decreased risk for kidney stones. It does not addresses latté or triple caramel Frappuccino. So, as always drink coffee in moderation.
Download Your Copy!
One in every 5 CKD patients receives a nephrotoxic medication
This study published ahead of print looked into the use of nephrotoxic medications in the US and Sweden. They studied a total of 74,135 patients with stage 3-5 CKD. In one year, one in every 5 patients with CKD, received a nephrotoxic medication.
Subscribe here to receive a FREE monthly update on the latest research in Integrative Nephrology straight to your inbox.
The post November Research and News appeared first on Integrative Kidney.]]>
Metformin and CKD survey results
You can see the results of the survey in this earlier blog. It demonstrated that caution about the use of metformin in CKD is common among primary care physicians and other specialties. Nephrologists seem to be more comfortable with using it until the patient reaches stage 4 CKD. Most nephrologists, however, were not aware that metformin is associated with nutritional deficiencies. You can read the results of the survey in detail here.
What is metformin?
Metformin was first produced in 1922. However, since 1958 it has been used in the control of blood sugar in type 2 diabetes. It is a biguanide drug, a class of medications that inhibit the liver’s production of glucose, enhancing the body’s insulin sensitivity and lowering the amount of blood sugar that the intestines absorb. It is chemically developed from galegina, a natural guanidine compound found in Galega officinalis (French lilac, also known as goat’s rue).
In essence, metformin is an oral diabetes medication that helps control blood sugar levels. It is often used together with diet and exercise to improve blood sugar control in patients with type 2 diabetes mellitus. There are other off-label uses for metformin and it is currently being studied for the treatment of polycystic kidney disease.
Join us in the fight against kidney disease and receive the FREE Report “5 Pitfalls to Avoid When Caring for Kidney Patients”
Does metformin cause acute kidney injury?
For many years clinicians have been avoiding the use of metformin in kidney patients and specifically in those with diabetes. This is fueled by the FDA warning about the use of metformin in these patients due to concerns about lactic acidosis (discussed later). The original FDA warning was much more strict, but the more recent one issued in 2016 weighed in with more detail about metformin and kidney function. The new warning allows metformin to be used in patients who have worse kidney function. The newest warning indicates metformin can be used in patients who have an estimated glomerular filtration rate (eGFR) greater than 45 mL/min. Furthermore, metformin can continue to be used in existing patients whose eGFR remains over 30 mL/min.
As you saw from the survey, many primary care physicians and other specialists think that metformin can cause direct acute kidney injury. However, the literature shows that metformin can be protective in kidney disease. There is absolutely no evidence that metformin can lead to kidney injury. In fact, there is evidence to the contrary.
Download Your Copy!
Metformin clearance by the kidneys
Metformin does not undergo metabolism in the body, and it is eliminated unchanged in the urine. It is mainly cleared by tubular secretion in the kidneys. Metformin clearance is proportional to creatinine clearance. Therefore, although metformin can be used in patients with advanced kidney disease the dose of metformin should be decreased. The following table shows the recommended doses of metformin according to kidney function.
| Kidney function | Total daily metformin dose |
| Normal | 3000 mg |
| 45-59 ml/min | 2000 mg |
| 30-44 ml/min | 1000 mg |
| Less than 30 ml/min | Not recommended |
Metformin-induced diarrhea
The most common side effects of metformin are gastrointestinal. This is because one of the ways that metformin works is directly on the gut, altering glucose (sugar) absorption in the gut. Consequently, symptoms of nausea and diarrhea can occur especially in the first few weeks of taking it. That is why the patient should be started on a low dose to get used to it. Despite the statistic that 25% of patients taking metformin report diarrhea, only about 5% of those taking it had to stop it due to that side effect.
Metformin and lactic acidosis
The real reason why metformin was technically “banned” from use in CKD patients in previous years was due to the development of lactic acidosis. Lactic acidosis is a disease where lactic acid, a metabolic byproduct, accumulates in the blood. Lactic acid is mainly produced in small amounts by the muscles and red blood cells. It is formed when the body breaks down sugars to make energy under conditions of low oxygen (anaerobic glycolysis). This can occur during intense exercise or severe infection (called sepsis).
Metformin can induce lactic acidosis by shifting energy production in the cells toward anaerobic glycolysis. It also decreases the ability of the liver to consume lactic acid. Yet, in practice this is rare. In fact, it has been shown that lactic acidosis can occur in patients taking other oral blood-sugar-lowering medications at the same rate as metformin. Most case reports of metformin-induced lactic acidosis were in patients who have other conditions that lead to acute kidney injury (AKI) and lactic acidosis such as septic shock.
So, it is not that:

Instead, what happens is:

Finally, in a large retrospective study of patients with diabetes mellitus, metformin use was not significantly associated with lactic acidosis at kidney function levels higher than 30 ml/min/1.73 m2 (stage 3 or better).
Metformin and vitamin B12 deficiency
The association between long-term use of metformin and low vitamin B12 levels in type 2 diabetes mellitus patients is well-established. This is thought to be due to changes in the production of intrinsic factor in the stomach, which decreases vitamin B12 absorption in the intestine. Vitamin B12 deficiency is more pronounced if the patient is also taking a proton pump inhibitor such as omeprazole or histamine H2 receptor antagonist such as famotidine, which are medications used to treat acid reflux. Since diabetes can cause peripheral neuropathy, as well as vitamin B12 deficiency, can cause peripheral neuropathy, it can be confusing for diabetic patients on metformin and their practitioners.
Therefore, patients using metformin for a prolonged period should be screened initially and periodically for vitamin B12 deficiency. In addition, there is also growing evidence that other B vitamins, vitamin D, and magnesium can be impacted by metformin.
Bonus: Metformin’s impact on the gut microbiome
Because of metformin’s actions on the gut, it can also alter the intestinal microbiota for the better. Studies showed that metformin can enhance the growth of Akkermansia muciniphila, Butyrivibrio, Bifidobacterium, and Lactobacillus. In addition, it decreases the levels of some other bacteria like Intestinibacter. Metformin also promotes the production of the short-chain fatty acids that protect the intestinal barrier. In fact, some authors attribute some of metformin’s actions to its favorable impact on the gut microbiota and integrity.
The Bottom Line for Metformin and Kidney Disease
The answer to the question “Is metformin bad for the kidneys?” is generally no. Metformin can be used in patients with kidney disease. It actually leads to better outcomes in these patients. However, the risk of metformin-induced lactic acidosis increases in CKD stage 4 and above. It is, therefore, not recommended for use in these patients and patients with acute kidney injury. I also recommend avoiding it in patients with renovascular disease because their kidney function tends to fluctuate. Furthermore, metformin can be associated with vitamin B12 deficiency and patients should be screened initially and periodically for deficiency of this important vitamin.
The post To Metformin or Not To Metformin in CKD appeared first on Integrative Kidney.]]>While this is not official medical research, I aimed to identify current thoughts among nephrologists and primary care providers about its use in CKD patients. The survey results suggest that many practitioners avoid metformin in CKD based on outdated FDA guidelines. In fact, metformin has beneficial effects for kidney health and can safely be used in certain stages of CKD. In this blog, I will share the survey results. For the current evidence and recommendations for metformin use in kidney disease, read the second part of this blog, “To Metformin or Not to Metformin in CKD.”
Participants in the Metformin and Kidney Disease Survey
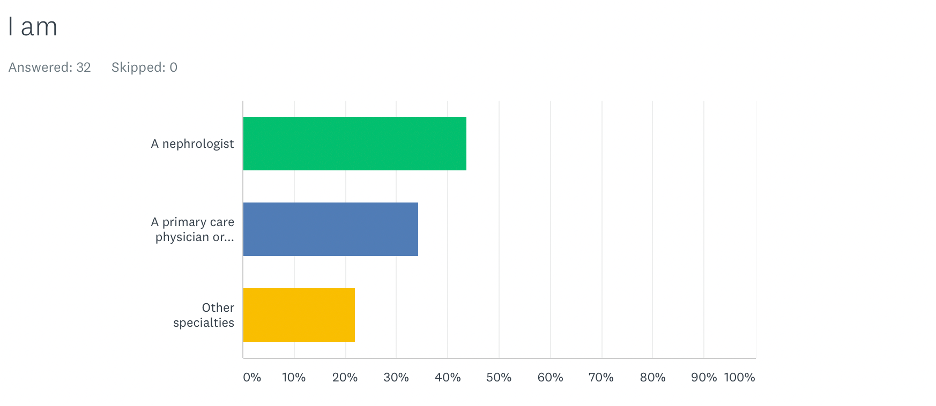
We had 32 respondents: 44% of the respondents were nephrologists, 34% were primary care physicians, and 22% were from other specialties.
Join us in the fight against kidney disease and receive the FREE Report “5 Pitfalls to Avoid When Caring for Kidney Patients”
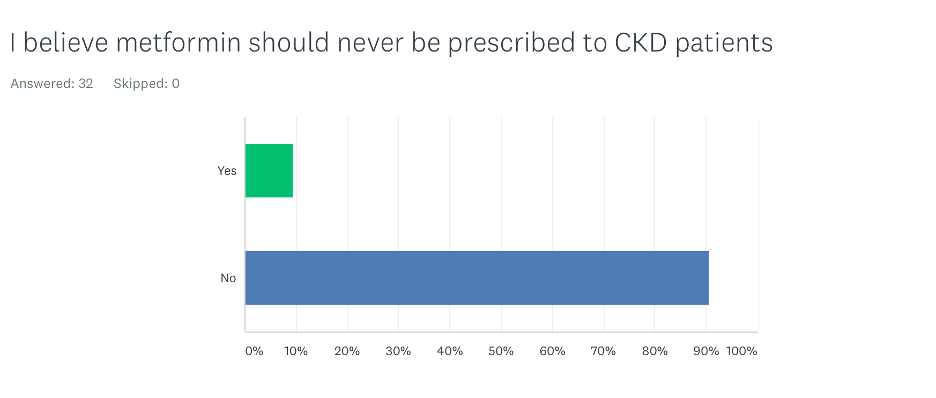
Should metformin be used in kidney disease patients?
Only 9% of participants thought that metformin should never be used in all CKD patients. All nephrologists believed that metformin can be used in patients with CKD. Among primary care providers, 27% believed that metformin should never be used in all CKD patients.
Does metformin cause acute kidney injury?
In the survey, 28% of participants believed that metformin causes acute kidney injury. The majority of those were primary care physicians. Only 7% of nephrologists believed that metformin causes acute kidney injury.
Block "fundamentals" not found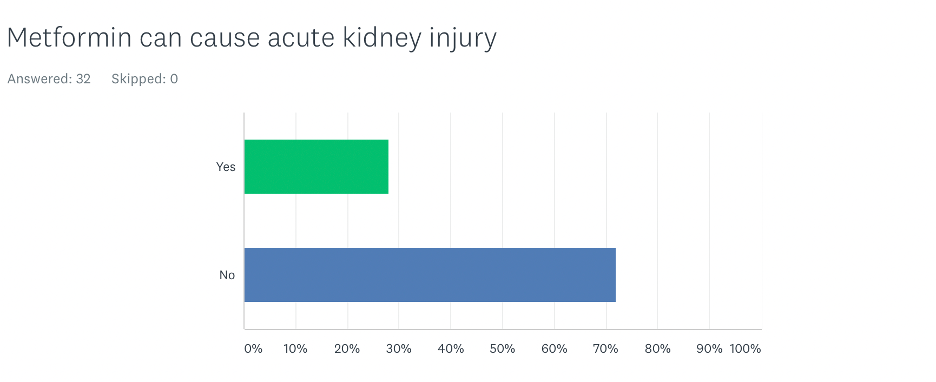
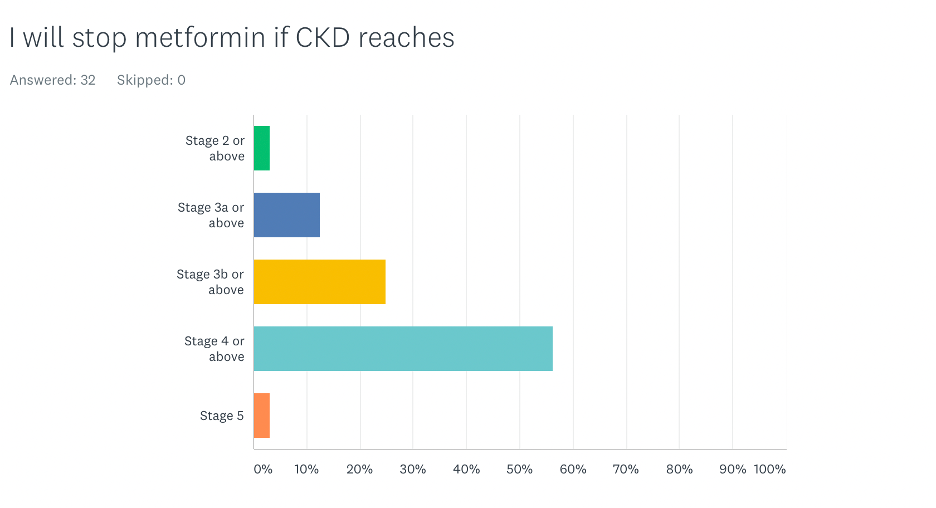
At what stage of CKD do you stop metformin?

The majority of participants (56%) believed that metformin should be discontinued when a patient reaches stage 4 CKD or above. Interestingly, 25% of the participants recommended discontinuing it if the patient reaches stage 3b CKD. Most nephrologists discontinued it when patients reached stage 4 CKD or above. Most physicians who discontinued it at earlier stages were primary care physicians.
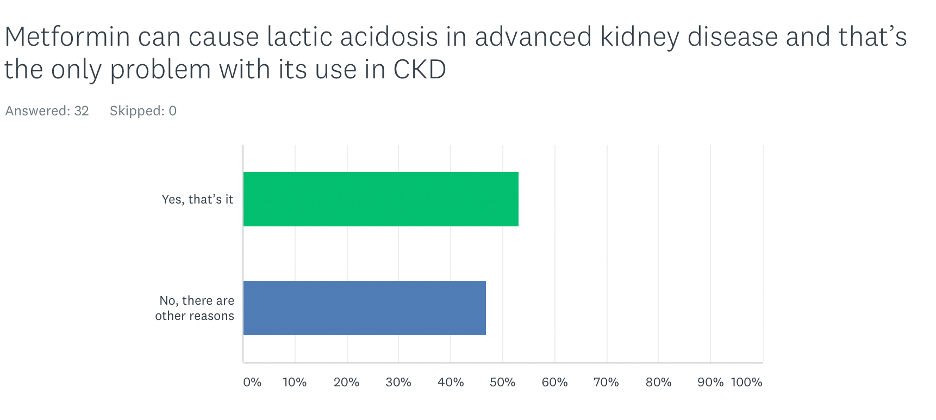
What is the problem with the use of metformin in advanced kidney disease?
This question may be suggestive, but about half of the participants believed that the risk of lactic acidosis is the only problem with the use of metformin in patients with advanced CKD. Interestingly, the majority of participants who believed there are other problems with the use of metformin in advanced kidney disease were non-nephrologists. One would think that nephrologists would be more aware of other risks beyond lactic acidosis.
When asked about specific reasons to avoid using metformin in advanced CKD, two rationales mainly emerged. Because metformin is removed from the body by way of the kidneys, one reason for its avoidance is the potential accumulation of excessively high levels of metformin in advanced kidney disease. The other reason was that metformin can be associated with diarrhea that can lead to volume depletion (loss of body fluids) and acute kidney injury.
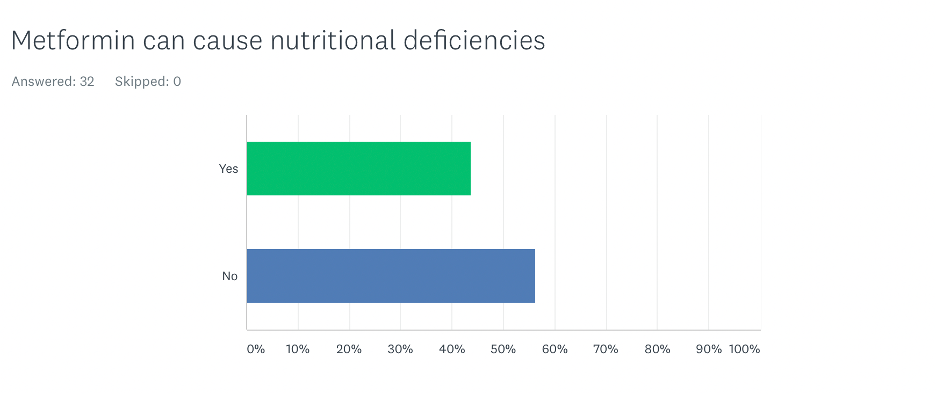
Can metformin cause vitamin B12 and other nutritional deficiencies?
Strikingly, 56% of participants were not aware of metformin and vitamin B12 deficiency or that it may cause depletion of other nutrients. Among nephrologists, this percentage was an amazing 79%.
The Bottom Line
Caution about the use of metformin in CKD is common among primary care physicians and other specialties. Nephrologists seem to be more comfortable with using it until the patient reaches stage 4 CKD. Most nephrologists, however, were not aware that metformin is associated with nutritional deficiencies. In the next blog, I will dig deeper into the research to find evidence-based answers to the questions presented in this survey.
Download Your Copy!
Types of Stress
Generally speaking, there are three types of stress:
- Major catastrophic life events that require considerable behavioral modification such as the death of a loved one, divorce or loss of a job.
- Chronic strains that are persistent stressors which require some adjustment over a long period of time such as poverty or disability.
- Daily hassles that occur over the course of the day such as traffic issues or unpleasant personal interactions.
The way people perceive and handle stress varies from person to person, with some people better equipped to handle stress than others. Certain factors, which we detail below, impact a person’s ability to cope with stress. These include genetics, environment, and in utero exposure. Furthermore, previous traumatic life experiences may affect future handling of stress in an individual.
Most of the early literature on stress focused on the first two types listed above, but research is now looking at the third type and its effect on health.
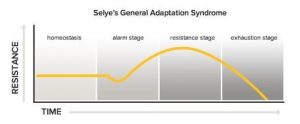
According to Selye, there are three phases of behavioral adjustments to stressors. The first phase is the alarm stage in which a person will have a “fight or flight” response. If the stressor persists, the person enters into the resistance or adaptation stage. Finally, long term exposure to the stressor will eventually lead to the exhaustion stage.
Factors that influence stress
Although we all experience stress, some individuals are better suited to handle stress than others. There may be some individual variability due to various genetic and environmental factors, as well as the impact of trauma and adverse childhood experiences.
Genetics
Small differences in our genes, called single nucleotide polymorphisms (SNPs), can affect our hormonal responses and enzymes that are associated with psychological responses. One example is a SNP in catechol-O-methyltransferase (COMT) gene which produces an enzyme that breaks down dopamine, epinephrine, and norepinephrine (neurotransmitters associated with the fight-or-flight response). Mutations in the way this gene is expressed, can lead to an increased stress response.
Another example is a protein called brain-derived neurotrophic factor (BDNF) which protects and improves signaling between brain cells. Any SNPs in BDNF or its receptors can decrease resilience to stress. In fact, the impact of stress on BDNF has been strongly associated with affective disorders.
Environment
The area and physical environment where a person lives and works can be a stressor. Environmental stressors such as living in disadvantaged neighborhoods, limited access to supermarkets, residential density, availability of recreational resources, and distance to wealthy areas, are associated with the development of insulin resistance, type 2 diabetes, obesity, and cardiovascular disease, all of which are risk factors for CKD. It is important to know this is subjective and environmental stressors for one individual may not be stressful to another.
In Utero Exposure
The stress a woman experiences during pregnancy can greatly impact the development of the baby while in utero, leading to lifelong complications. Prenatal stress has been shown to affect hypothalamic-pituitary-adrenal (HPA) axis programming of the fetus, making it more difficult for the offspring to handle stress in the future. Furthermore, this altered HPA activity has been linked to low birth weight which may result in a decrease in nephron endowment (the number of filtering units the baby is born with), as well as metabolic syndrome and cardiovascular disease, known risk factors for CKD.
Nutrition as a Stress Mediator
Research suggests that some nutrients can heighten the response to stressors while other nutrients relieve it. For example, magnesium and zinc can help a person feel more calm. In addition, omega-3 fatty acids and foods high in probiotics can reduce stress and anxiety. On the other hand, caffeine can make a person feel anxious. It is important to note that genetics play a role in caffeine metabolism and its effects.
Indirect Effect of Stress on the Kidney
Stressors can lead to changes in the hypothalamic-pituitary-adrenal axis (HPA axis) and neuroendocrine hormones. These changes are associated with increased cortisol levels, increased epinephrine, and inflammatory cytokines which are linked to the development of insulin resistance, metabolic syndrome, high blood pressure and type 2 diabetes.
Direct Effect of Stress on the Kidney
Studies have shown that the sympathetic system innervates all segments of the kidneys including the blood vessels and tubules. Stimulating the sympathetic system can affect blood flow to the kidneys and lead to sodium retention at the level of the tubules, resulting in the progression of kidney disease.
The Vicious Cycle
As we have seen above, epinephrine and norepinephrine can play a role in the psychological stress response on the kidneys. These neurotransmitters are usually broken down in our bodies by two major enzymes: monoamine oxidase (MAO) and COMT. Recently, a new enzyme, renalase, was found to be produced by the kidneys and involved in the breakdown of these neurotransmitters.
Renalase is a flavoprotein that metabolizes catecholamines (epinephrine, norepinephrine, and others) to aminochromes. It utilizes NADH as a cofactor. Therefore, deficiencies in vitamin B2 and B3 can affect its function. Studies have shown that renalase levels in the blood correlate with normal kidney function and kidney mass. Decreased level of renalase leads to elevated blood pressure and heart rate, physiological responses to stress. Furthermore, it’s been shown that decreased levels of renalase increase the sensitivity of the heart and the kidneys to ischemia (decreased blood flow).

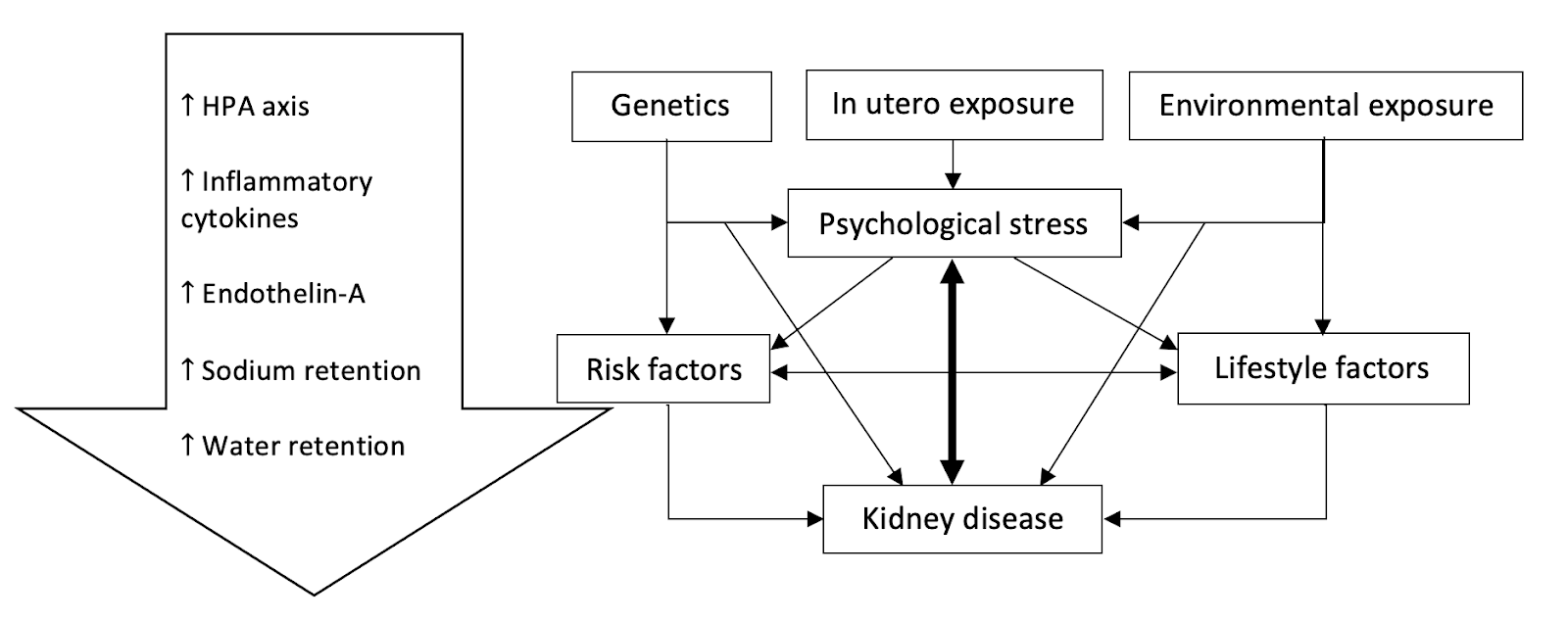
This creates a vicious cycle in which stress causes kidney disease and the latter, in turn, amplifies the effect of stress on the body.
In essence, the interplay between stress and kidney disease can be summarized in this diagram.
The Bottom Line
Our increasingly stressful lives can lead to increased cortisol levels, insulin resistance, and inflammation. Stress has been linked to increased levels of epinephrine and norepinephrine. These changes lead to the development and progression of kidney disease. Genetics, environment, and nutrition all play important roles in augmenting these changes. It’s essential that a stress management practice is part of a comprehensive Integrative and Functional Medicine approach to kidney health.
The post Stress and kidney health appeared first on Integrative Kidney.]]>

Sex-specific Associations of Sex Hormone Binding Globulin with CKD and Kidney Function: A Univariable and Multivariable Mendelian Randomization Study in the UK Biobank
Do sex hormones play any role in the progression of kidney disease? It has been long observed that CKD is more prevalent in women; however, the progression of CKD is much faster in men. This study looked at the sex hormone binding globulin (SHBG) using Mendelian randomization. Higher SHBG levels were associated with lower risk for CKD and better renal function in men but not in women. “Identifying factors affecting SHBG, and underlying pathways, could provide new insights for prevention and treatment strategies.”
https://jasn.asnjournals.org/content/32/3/686
Water intake and progression of chronic kidney disease: the CKD-REIN cohort study
How does water intake affect the progression of kidney disease? In this study, researchers found that “in patients with CKD, the relation between plain water intake and progression to kidney failure appears to be U-shaped. Both low and high intake may not be beneficial in CKD.”
Anti-neutrophil cytoplasmic antibody associated glomerulonephritis complicating treatment with hydralazine
Medications can sometimes be triggers to autoimmune kidney diseases. This article talks specifically about hydralazine which is an old blood pressure medication that is used often by our cardiology colleagues specifically in patients with advanced kidney disease who are often not candidates for ACE inhibitors or ARB therapy.
https://www.kidney-international.org/article/S0085-2538(21)00379-3/fulltext?WT_MC_ID=ITL
The post May Research and News appeared first on Integrative Kidney.]]>