
Causes of magnesium deficiency
Poor dietary choices
There has been a steady decline in magnesium content in cultivated fruits and vegetables over the past 100 years. This is caused by the depletion of magnesium in soil over time. In addition, utilizing phosphate-based fertilizers leads to the formation of magnesium phosphate salts that are not soluble. This means the soil is deprived of both components: magnesium and phosphorus.
On top of that, the rise of ultra-processed food and drinks have also contributed to the depletion of magnesium in the modern standard American diet. Grain bleaching and vegetable cooking and adding preservatives can lead to a significant loss of magnesium content. Preservatives such as various forms of phosphate and oxalate can bind with magnesium and prevent its absorption. Phosphoric acid in soft drinks has similar effects.
The addition of fluoride to drinking water also prevents magnesium absorption by binding to it and forming insoluble complexes. Finally, drinking caffeine and alcohol can also lead to an increase in the excretion of magnesium by the kidneys, causing magnesium deficiency.
Drug-induced magnesium deficiency
Many medications can interfere with magnesium absorption or increase its excretion, leading to deficiency. Most of the medications leading to magnesium deficiency are summarized in the following table:
| Medication class | Example | Mechanism |
| Anti-diabetic medications | Insulin, insulin mimetics | Interferes with Na/Mg exchange leading to renal loss |
| Antimicrobial | Gentamicin, pentamidine, foscarnet, amphotericin B | Increased renal loss |
| Beta agonists | Salbutamol | Renal loss and cellular shifts |
| Bisphosphonate | Pamidronate | Renal loss |
| Cardiac glycoside | Digoxin | Increased renal loss |
| Chemotherapy agents | Cisplatin | Renal loss |
| Diuretics | Thiazide diuretics | Renal loss |
| Proton-pump inhibitors | Omeprazole | Decreased GI absorption |
Measuring magnesium status
Simply put, there is no ideal test for assessing magnesium status in the body. Mg blood levels are tightly controlled and represent only 0.8% of total body stores (0.5% in red blood cells and 0.3% in the serum). Red blood cell Mg levels have been used as an alternative method, but this too does not represent total body stores and is not well validated. Measuring urine Mg requires measuring a 24-hour urine specimen. This too has been found to be imperfect due to large variations from day to day.
The Mg retention test has been proposed as a more accurate way to assess Mg status. Here, the patient receives an intravenous Mg load (0.25 mmol magnesium/kg body weight at a rate of 2.5 mmol/hour), and a 24-hour urine specimen is collected before and after the load. The percentage of administered magnesium that is retained by the body (not excreted in urine) determines magnesium status. This test is not standardized yet, but retention of 25%-50% may indicate a moderate deficiency, and retention of more than that may indicate severe deficiency.
Ideally, measuring muscle or bone magnesium may be more reflective of accurate magnesium stores but this is obviously not practical. Combining a serum Mg test, a 24-hour urinary Mg, and assessing dietary Mg intake is the most comprehensive and practical evaluation of a patient’s magnesium status.
Combining a serum Mg test, a 24-hour urinary Mg, and assessing dietary Mg intake is the most comprehensive and practical evaluation of a patient’s magnesium status
Share on X
Patients at high risk for magnesium deficiency include:
- Diabetics
- Heart disease patients
- Osteoporosis patients
- People who eat a diet high in processed food and soda
- People who suffer from leg cramps
- People with metabolic syndrome
- People who take certain medications
Those patients at risk of magnesium deficiency should be targeted for additional testing and supplementation.
Download Your Copy!






What type of magnesium should I take?
The type of magnesium supplement used depends on the exact indication. Magnesium supplements are available as oxide, hydroxide, gluconate, chloride, citrate, lactate, malate, taurate, L-threonate, sulfate, glycinate, orotate, and carbonate salts. In addition to magnesium citrate’s direct effects on kidney stones, magnesium benefits the person with kidney disease through its effects on blood pressure, insulin sensitivity, vascular health, and bone. The following indications are listed with the recommended types of magnesium supplements and doses. These doses are for prevention only. Patients who are deficient may need higher doses. Magnesium supplements should be discontinued or decreased in kidney patients if the serum magnesium level is higher than 2.6.
| Indication | Mg type | Dose |
| Prevention of kidney stones | Magnesium citrate | 400 mg daily |
| Bone health | Magnesium citrate or chloride | 400 mg daily |
| Improving blood pressure | Magnesium taurate | 400 mg once or twice daily |
| Improving insulin sensitivity | Magnesium taurate | 400 mg once or twice daily |
| Improving vascular health | Magnesium glycinate or orotate | 200-400 mg daily |
| Phosphate binder | Magnesium carbonate | 250 mg with meals |
We recommend using high-quality supplements. This article can be a useful guide.
The bottom line
Magnesium is essential to many biological functions, as I described in part one, “Magnesium and Kidneys.” It has many health benefits for kidney, bone, and vascular health. Assessing magnesium status is difficult but magnesium deficiency is very common and underrecognized. Supplementing magnesium may be important for patients with kidney disease. The type of supplement used depends on the indication. As always, it is recommended that you check with a Functional or Integrative Medicine provider and nephrologist before taking any new supplement.
The post Magnesium Deficiency: Assessment and Management for Better Kidney Health appeared first on Integrative Kidney.]]>By Lara Zakaria, PharmD, CNS, CDN, IFMCP
Kidney stone formation (also called urolithiasis or nephrolithiasis) is a complex disease influenced by multiple factors including diet, genetics, and environment. Anyone who’s experienced them can attest that stones are often very painful. When left untreated, they may contribute to more serious conditions including urinary tract obstruction and permanent kidney damage or CKD.
Read more about the etiology and prevalence of kidney stones here.
Conventionally, the approach to treatment is a multi-pronged approach and may include medication, dietary and lifestyle interventions, surgical removal, and using ultrasonic waves to break up stone. However, dietary guidelines tend to focus on stone composition instead of on the underlying pathology. In this series, we’ve been discussing the combination of upstream risk factors that impact risk of stone formation.
Factors that impact the integrative approach to kidney stones include:
- Type of stone
- Environment
- Diet
- Hydration and electrolyte balance
- Microbiome and gut health
- Genetics
Diet is a topic that deserves a deeper dive! We’ll focus on it here today.
Dietary Approach to Kidney Stone Prevention
The Diet Controversy and Kidney Stones
Dietary interventions are common in addressing kidney stones. The reality is, we need a more comprehensive approach when it comes to preventing kidney stone formation and kidney damage. Dietary approach to kidney stone prevention is one aspect of this comprehensive integrative approach.
First, let’s start by outlining the impact of the standard American diet (SAD), which seems to increase risk of kidney stone formation. When we use the term SAD, we are generally referring to a diet that includes:
- Consumption of sugary beverages and soda (and high carbohydrate consumption in general)
- Increased intake of processed/refined foods like cereals, crackers, baked goods, etc.
- Processed, fried, conventionally raised, high-nitrate animal protein
- Low intake of fiber and fresh produce in general
- A “beige” diet (low in phytonutrients and antioxidants) lacking color and low in enough variety of colorful fruits and vegetables
- Inadequate amounts of healthy, anti-inflammatory fats, and high amounts of refined unhealthy fats
Interestingly, studies have shown that eating more fresh produce is protective from kidney stone formation. When we consider that the SAD is low in protective foods and the key nutrients found to be helpful in preventing urolithiasis. Let’s examine these factors that impact kidney stones in more detail.
Macronutrient Balance for Kidney Stones (Protein, Fat & Carbs)
Protein
For a long time, it was assumed that stone formation was at least in large part due to excessive protein intake. As a result, those at risk for stone formation were instructed to eat a low protein diet to prevent urolithiasis. However, there are underlying factors that cause a domino effect impacting how the products of protein breakdown lead to stone formation. This includes micronutrient and electrolyte balance, metabolic disorders, digestive abnormalities, and of course dysbiosis (we’ll discuss these in detail in another blog).
It’s true that excessive protein intake can lead to more acidic urine and increased uric acid production (a risk factor for uric stone formation). Elevated protein metabolism alone isn’t a problem in isolation, there’re other upstream factors to consider that make certain individuals more susceptible to stone formation. Furthermore, the source of protein seems to be significant. Animal protein sources seem to play a bigger significance in risk of stone recurrence, while plant-proteins might be protective.
Carbohydrates and Fiber
Though excessive consumption of carbohydrates isn’t recommended, excessive restriction of carbs in people prone to kidney stones should be avoided. We suggest avoiding sources of simple sugars, fructose and high fructose corn syrup (that includes sugar sweetened beverages, pastries, sodas, and even the so-called healthy sweetener agave). Fructose consumption in particular seems to increase production of excess uric acid and simultaneously reduces its excretion in the urine.
Instead, we want to opt for more nutrient-dense, high-fiber, low-glycemic carbohydrates, including root vegetables, berries, whole grains and legumes. Increased consumption of fiber helps to promote improved microbiome health and diversity, which may play a significant role in kidney stone formation risk. Furthermore, there is interesting research that indicates that individuals who aren’t getting enough dietary vitamin C to meet their needs while on a low-carb diet may increase their risk for developing certain types of kidney stones.
This begs the question, what other nutrient deficiencies might contribute to stone formation when macronutrients might not be optimized?
Fats and Essential Fatty Acids
In order to balance a moderate protein and carb intake, some individuals might benefit from increasing calories from fat. Healthy fats include omega 3 sources like fish and fish oil, nuts, seeds, olive oil, and avocado. Grass-fed ghee might be especially beneficial due to a combination of anti-inflammatory profile, vitamin A, and gut healing benefits of the butyric acid component.
Independently, increased fat intake has not been associated with kidney stone formation. However, when coupled with a SAD diet full of simple carbohydrates and fried and processed foods, and excessive protein intake that seems, at least in part, to be a contributing factor. At the same time, when eating a high-fat diet as part of a ketogenic approach, excessive restriction of carbohydrates seems to contribute to stone formation in individuals with existing risk factors. In those cases, it’s recommended to work with a nutritionist to ensure that you’re balancing your macronutrients effectively to avoid kidney stones.
Micronutrient Balance
Fat-soluble vitamins
We can’t talk about dietary approach to kidney stone prevention without discussion fat soluble vitamins. Fat soluble vitamins include vitamins A, D, E, and K. Deficiencies in D, A and K in particular have been associated with kidney stone formation. This might at least in part be due to the fact that these vitamins play a major role in calcium metabolism and bone mineralization. When D and K are deficient, calcium from diet is deposited in arteries instead of in bones, leading to calcification and stone formation.
In fact, vitamin K depletion might be an independent risk factor for kidney stone formation. When individuals form kidney stones, a vitamin-K dependent protein (matrix Gla protein) is secreted in inactive form. This protein when activated with vitamin K can inhibit the growth of calcium oxalate crystals. When vitamin K isn’t available, more crystals may form.
To improve dietary intake of these nutrients, foods like eggs (especially the yolks), organ meats, ghee, natto (fermented soybeans), and full-fat cheeses (assuming you’re able to tolerate dairy) can be helpful to include in your diet. Daily sun exposure (at least 20 minutes a day) can also help promote increased vitamin D levels. However, supplementation is often indicated. Issues with absorbing fats and fat-soluble vitamins due to digestive issues are common, a nutritionist or a clinician trained in Integrative and Functional Medicine can help you determine if supplementation is needed.
Oxalates
Oxalates are front and center in the dietary approach to kidney stone. In fact, calcium oxalate stones comprise most kidney stones (75%). There’s some evidence that limiting consumption of oxalates can help reduce stone formation. Food containing high levels of oxalates tend to be generally considered healthy, including spinach, beets, nuts and seeds, to name a few examples.
What makes these foods healthy for some people, and contribute to stone formation in others?
One reason might be inadequate calcium intake from the diet. Food sources like broccoli, sardines and canned salmon, and leafy greens like kale and collard greens can be good low-oxalate, calcium-rich food sources. When consumed in adequate amounts, calcium binds to oxalates in the intestines, preventing it from being absorbed and reducing formation of stones.
Another important consideration is the composition of the microbiome. When oxalate-degrading bacteria in the gut is inadequate, it can increase risk of developing kidney stone disease. More about that in a future article.
Vitamin C
Ascorbic acid has been associated with formation of kidney stones. Excessive intake of vitamin C might increase oxalate production. Some studies have shown higher intake of vitamin C is associated with increased risk of kidney stones, but only in people predisposed to forming oxalate-stones. Regardless, caution should be used in supplementing vitamin C within the context of the larger, integrative picture.
Phytate
Phytate, sometimes called phytic acid, is an antioxidant compound found in certain foods like beans, lentils, nuts, and seeds. Some have claim that phytate intake might prevent the absorption of certain nutrients, but actually it might be protective for kidney stone! One study found that women who consumed more phytate had reduced risk of kidney stone formation. Other studies have come to the same conclusion. This might account to the benefit of eating these particular foods, which happen to be good plant-based protein sources, in place of animal protein.
Salt and Other Electrolytes
Calcium is a controversial topic when it comes to risk of kidney stone formation. Surprisingly, higher intake of dietary calcium (from food sources like leafy greens, salmon, and legumes, for example) is associated with lower risk of stone formation. On the other hand, taking calcium supplements may be linked with increasing risk of kidney stone formation (this might be gender specific to men).
Furthermore, the conversation often fails to address the nuance of calcium consumption in the form of dairy, which might not be superior over plant-based forms of calcium, or to account for the impact of vitamin D deficiency.
Magnesium is another electrolyte that is often overlooked. Magnesium is part of hundreds of the body’s biochemical reactions, so adequate intake is essential. Furthermore, ensuring adequate intake of magnesium can help prevent the formation of calcium oxalate stones by destabilizing the bond between the two compounds causing them to split.
Food sources of magnesium include swiss chard, spinach, almonds, and pumpkin seeds. Many of those foods might be contraindicated in a low-oxalate diet, so supplementation might be indicated before gradually adding those foods back as part of a comprehensive approach. Supplementing with chelated forms of magnesium (like magnesium citrate, malate, or bisglycinate) or making time for an epsom salt bath (magnesium sulfate in the salts absorbs through the skin).
But the most important electrolyte in the dietary approach to kidney stone is sodium. Excessive sodium (salt) consumption has been associated with stone formation, particularly when fluid intake is inadequate. High sodium excretion increases calcium deficiency by increasing excretion through the urine. Reducing excessive intake of sodium, especially from processed foods like cured meats, can be helpful, along with ensuring adequate intake of potassium-rich foods like broccoli, leafy greens, squash, potatoes, mushrooms, bananas, cantaloupe, and grapefruit to name a few.
More about the impact of electrolyte balance on kidney stone formation in a future blog.
Water (the forgotten macronutrients)
Inadequate water intake is one of the most significant contributing factors to kidney stone formation. The process of excretion of oxalate consumes salt and water, as a result dehydration is more likely.
Taking mineral compounds containing citrate (like magnesium citrate or potassium citrate) can prevent the formation calcium oxalate and uric acid stones while balancing mineral needs. Adding lemon juice or apple cider vinegar (4oz per day) to water might also help prevent urolithiasis through the same mechanism. Your Integrative or Functional Medicine clinician can help create a plan that best fits your needs.
The Bottom Line
Multiple factors impact kidney stone formation, including dietary factors. It seems there’s no single food or food component that causes stone formation. Rather, there are likely a combination of factors including nutrient depletion, dehydration, and poor food choices combined with environmental factors, genetics, and gut integrity and microbiome balance which combined play a role.
Therefore, the integrative approach to addressing kidney stones must account for the constellation of these factors. Practitioners working with individuals to prevent kidney stone formation should formulate a personalized approach that modifies all relevant components in their integrative approach. We’ll explore these connections in future blogs in this series.
The post Dietary Approach to Kidney Stone Prevention appeared first on Integrative Kidney.]]>
It has been suggested that it could be due to agricultural chemicals, heavy metal exposure, silica inhalation, infectious diseases, genetic predisposition. Many of these workers regularly work in hot conditions for long hours. More recently, they identified repeated heat stress as a cause and a risk factor for kidney disease.
There is no doubt that the prevalence of kidney disease is rising in the United States (US) and throughout the world. In fact, one in seven people in the US has kidney disease. It is one of the fastest growing causes of death throughout the globe. An estimated 5–10 million people die annually from kidney disease worldwide. Unfortunately, due to poor data, lack of awareness, early detection and access to care these numbers could underestimate the exact burden of kidney disease in the world.
Chronic Kidney Disease of Unknown Origin (CKDu)
The type of chronic kidney disease that affected the agricultural workers in Central America is now called chronic kidney disease of unknown origin (or CKDu). Since the nineties, CKDu has been identified in studies of similar etiologies in Siri Lanka, India, Africa, South America and the Middle East. The common thread is the hot and humid climate.
CKDu does not follow the conventional risk factors for kidney disease and, therefore, it’s challenging to detect early and prevent. It disproportionately impacts areas with underprivileged communities and poor infrastructure. However, it would be a mistake to assume that this problem is limited to developing countries. Acute kidney injury has been reported in agricultural workers exposed to hot conditions in California and Florida.
Primary Impact: Global Temperature & Kidney Injury
It has been documented that global temperature have increased by about 1 degree centigrade (1.8 degrees Fahrenheit) in the past 50-100 years. Scientists agree that these changes have contributed with record heat waves, melting ice caps and rising sea levels, and extreme weather patterns. This pattern is posing significant health risks, some directly and some indirectly.
According to a United Nations report, climate change is expected to exacerbate health problems that already pose a major burden to vulnerable populations including children and the elderly. Climate change has been associated with a rise in many infectious diseases, especially water-borne illnesses like cholera, typhoid, and dysentery. It is also expected to contribute to the chronic disease burden and bring on new health epidemics. Not surprisingly, CKDu is one of these health issues.
Secondary Impact: Kidney Disease, Pollution, Water & Food Security
So how does rising temperature affect kidney health? The evidence points to heat stress and dehydration can result in chronic kidney disease as playing an important role in the epidemic of CKD worldwide. In fact, the progression of kidney injury has been found to worsen with rising core body temperature.
The mechanism seems to be linked with a decrease in adenosine triphosphate (ATP) levels and reduced mitochondria. These energy powerhouses are particularly abundant in the kidneys, and with reduced ATP and mitochondria, oxidative stress and cellular damage increases. Combine that with a diet with low nutrient-density and inadequate antioxidant content to neutralize oxidative stress, and risk of CKD significantly elevates. In laboratory studies, the supplementation of antioxidants prevented rats who were exposed to heat stress from developing kidney injury.
Furthermore, heat has been associated with increased risk of kidney stones and kidney stones are known risk factors for kidney disease. Since the kidneys are major site for the metabolism and elimination of toxins, exposure to toxins such as glyphosate contributes to kidney injury due to oxidative damage. Glyphosate in particular also impacts dysbiosis and gut health, which may be a confounding factor in the equation when we consider the gut-kidney connection.
As droughts become a more frequent occurrence as a consequence of climate change, dehydration from heat exposure and inadequate water consumption can lead to concentration of these toxins and, therefore, amplification of their negative effects.
Another factor to consider is the increase of pollution like heavy metal, plastics, and chemicals like pesticides and herbicides. Contamination of air and soil with pollutants increases inhalation and ingestion through food, including rise of mercury contamination in fish and arsenic in rice for example. These toxins have been associated with the rise in incidence of KDas well as other chronic diseases like diabetes and hypertension.
Last but not least, as climate change impacts food security and farming practices, access to fresh food and produce might be compromised. This may shift consumption to processed foods with less nutrient value, including less vitamins, minerals, phytonutrients, and antioxidants needed to promote healthy kidneys. Increased consumption of processed foods also leads to reduced fiber consumption, which impacts gut health and the microbiome which might be the most significant factor as we’ve discussed in our blog on the gut-kidney connection.
Other Considerations
It may sound like a cliché, but hydration is key. For those in labor industries or who work in agriculture or at increased risk of extended heat and chemical exposure, extra effort should be made to adequately hydrate. Broader public health measure and policy should be put in place to improve worker safety.
The risk increases for those taking medications that:
· Increases risk for dehydration, including diuretics (furosemide, hydrochlorothiazide, etc) or SGLT-2 inhibitors (canagliflozin, dapagliflozin, etc), or
· Decreases circulation to the kidneys, including ACE inhibitors (lisinopril, captopril, etc), angiotensin receptor antagonists (ARBS like losartan, Olmesartan, etc). However, as we mentioned earlier, heat lead to energy depletion in the kidneys and supplementing with antioxidants may further decrease the risk of kidney injury due to extreme heat.
Bottom Line
Rising global temperatures are posing increasing risk for kidney disease and contributing to a worldwide rise in chronic kidney disease. Extended exposure to heat and dehydration can lead to kidney injury and kidney stones. Improved hydration, improved nutrient-density diet, and use of antioxidants maybe be preventive. Other confounding factors cannot be ignored, including increased environmental pollution, factors that impact on gut health, and medications. Although individuals can take steps to reduce our carbon footprint, but broad public health measures must advocate for policy changes that reduce contributions to climate change and the resulting global health impacts.
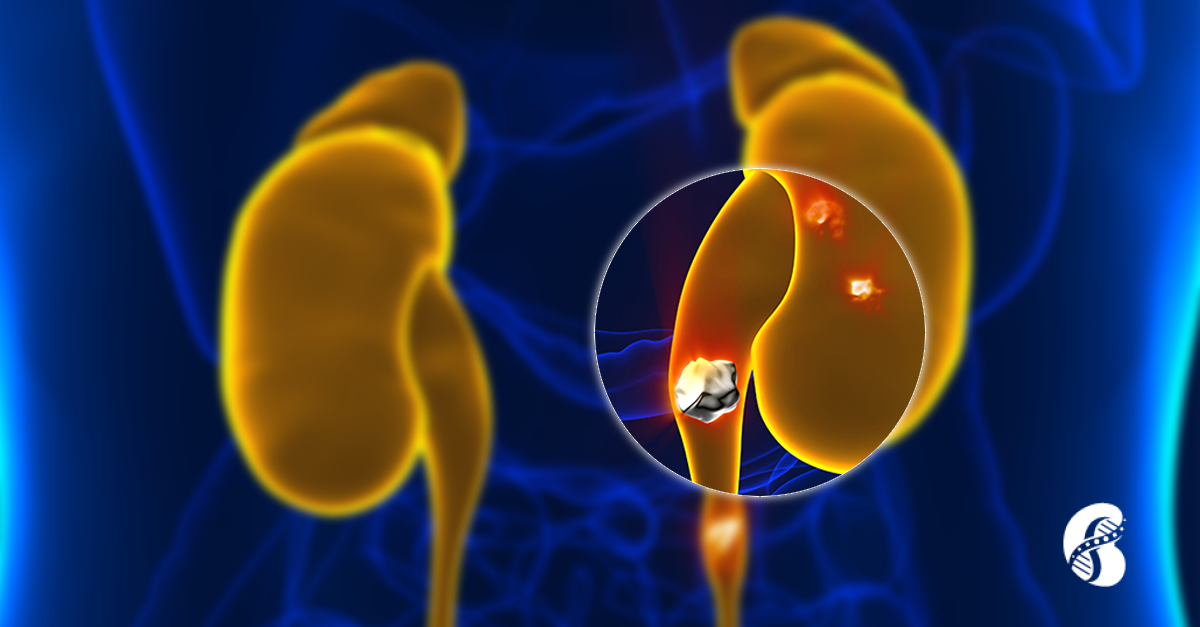
The post Impact of Climate Change on Kidney Health appeared first on Integrative Kidney.]]>Kidney stone, also called nephrolithiasis or urolithiasis, is a complex disease influenced by multiple factors including genetic and environmental factors. Stones are often painful, and left unaddressed can lead to more serious conditions such as obstruction of the urinary tract and permanent damage to the kidneys.
By Majd Isreb, MD, FACP, FASN, IFMCP
The frequency of kidney stones has been on the rise in the United States (US) according to nationally published data. The National Health and Nutrition Examination Survey (NHANES) has analyzed the health and nutrition status of the general populations for the past 30 years. According to analyses from these publications, the lifetime chance for developing kidney stone in an adult (age 20-74) increased from 3.2% in the 1970’s to 5.2% in the 1980’s. Most recent survey using data between 2007 and 2010 showed that the lifetime chance for kidney stones in an adult is now up to 8.8%. That’s almost a three-fold increase over three decades.
In addition to the inconvenience and pain associated with kidney stones, they also pose a significant healthcare burden and cost. Patients with kidney stones are likely to present to the emergency department and are often hospitalized for an average of 2-3 days. If patients cannot pass them, they may require surgical intervention. In 2000, the total costs for caring for patients with kidney stones in the US. was estimated at $2.1 billion. Furthermore, it is estimated that the cost of care will rise by $1.24 billion per year by 2030.
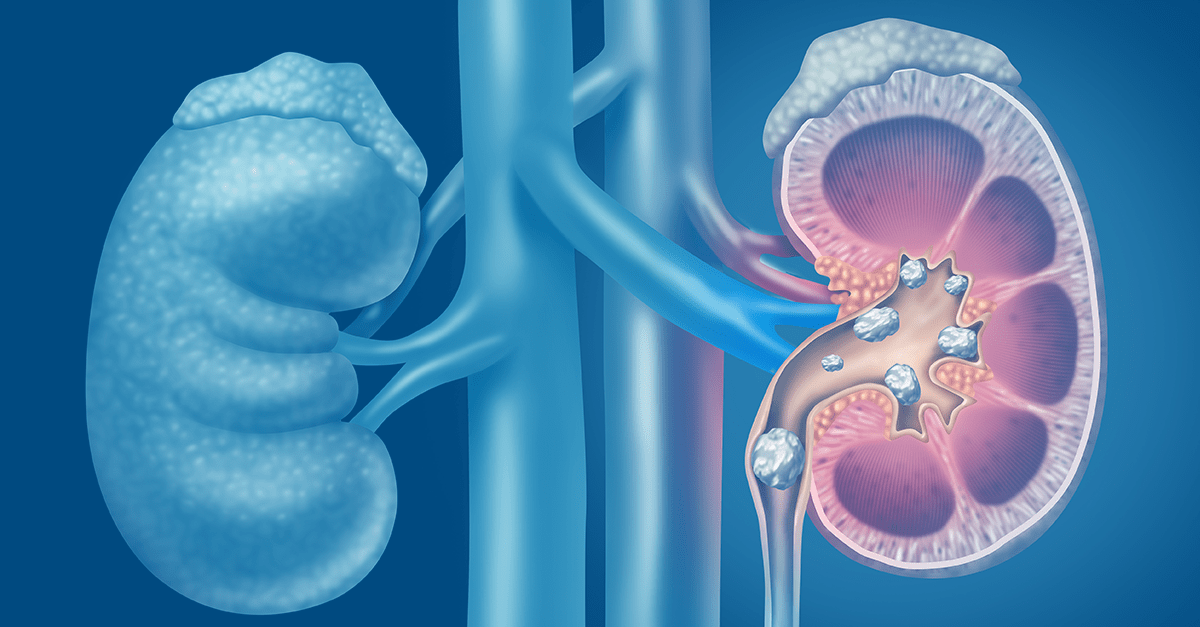
Kidney Stones: Types and Formation
There are five major types of kidney stones: calcium oxalate, calcium phosphate, uric acid, struvite (magnesium ammonium phosphate), and cystine. Calcium oxalate is by far the most common, comprising approximately 75% of kidney stones.
Calcium oxalate and calcium phosphate stones
Calcium stones are the most common type of kidney stones. They are composed of either calcium oxalate or calcium phosphate compounds. They are formed when calcium binds to oxalate (or phosphate) in the urine. On the other hand, dietary calcium can bind oxalate in the intestine and prevents its absorption through the gut, so there is less in the urine to form stones.
Oxalates are compounds found naturally in certain foods (nuts, spinach, potatoes, tea, and chocolate). In those prone to calcium oxalate formation, eating high amounts of foods rich in oxalates can increase the amount of oxalate in the urine and increase risk of stone formation.
Calcium phosphate stones are less common than calcium oxalate stones. Causes include hyperparathyroidism (when the body produces too much parathyroid hormone), renal tubular acidosis (a kidney condition that causes a buildup of acid in the body), and urinary tract infections. It is important to understand if one of these conditions is behind the formation of calcium phosphate stones.
Inadequate hydration is a major risk factor for these types of stones. Certain medications can also reduce risk of stone formation, including thiazide diuretics (for example, hydrochlorothiazide) reduce calcium levels in the urine available to form stones. Potassium citrate binds to calcium, preventing it from binding to oxalate and phosphate to form stones.
Download Your Copy!
Uric acid stones
Uric acid stones generally form when urine is too acidic, causing otherwise normal levels of uric acid to dissolve into the urine where it may crystallize forming stones. Therefore, by alkalizing the pH of the urine, we can prevent crystal formation.
In these cases, potassium citrate is the most common medication used to manage uric acid stone formation. Another medication, sodium bicarbonate can also be used to alkalinize the urine.
However, in some individuals, consumption of too much animal protein can actually increase the production of uric acid. In these cases, dietary restriction of animal protein might be necessary to manage excessive uric acid production. Use of allopurinol, a medication that prevents uric acid formation from precursors xanthine and hypoxanthine may also be indicated.
Struvite stones
Struvite stones are composed of magnesium ammonium phosphate, and unlike other stones, form in alkaline urine. Most commonly, these types of stones form due to a bacterial infection that raises the urine pH to alkaline levels. To dissolve these stones, acetohydroxamic acid (AHA) is used to reduce urine pH and ammonia.
Cystine stones (least common kidney stone type)
Cystine stone formation (also called cystinuria) is a relatively uncommon type of stone and the result of a genetic condition. As a result, urinary elevations of the amino acid cystine result in stone formation. Cystine stones can often be managed by improving hydration and maintaining alkaline urinary pH through diet and medication.
The Integrative Approach to Kidney Stones Treatment
Conventionally, the treatment approach may include a multi-pronged approach and may include medication, dietary and lifestyle, surgical removal, and using ultrasonic waves to break up stones.
There are a few conventional dietary guidelines, but guidelines tend to focus too far downstream, on stone composition, not on the underlying pathology and across risk factors upstream to prevent formation. By understanding the pathology and risk factors involved, we can better understand why some people develop stones, while others do not and effectively reduce the incidence of urolithiasis.
Socioeconomic and Environmental factors that impact the development of kidney stones
Studies of the distribution of kidney stones in the US suggest that geography is an important consideration in risk. For example, individuals who live in southern states, are more likely to have kidney stones than those who live in the North. In fact, inhabitants of the Southeast are nearly twice as likely to have a history of kidney stones as compared to those living in the Northwest. This has earned North Carolina, South Carolina, Georgia, Alabama, Mississippi, and Tennessee the nickname “the stone belt.”
Incidentally, these states also lead the nation in obesity and the incidence of diabetes. Inhabitants of these states are also more likely to consume a Standard American Diet (SAD) increasing the risk of pH imbalance that can lead to kidney disease and risk of stone formation.
Another factor to consider is climate. Higher ambient temperature and sunlight index are associated with a higher risk for kidney stones. Also, the incidence of kidney stones is higher in the summer than in the winter. This may in part explain why inhabitants of the warmer states in “the stone belt” have such a high incidence of kidney stone formation.
Why is this significant? Understanding this disproportionate distribution can help us understand the complexity of kidney stone pathology to better build a better approach. Our integrative approach to prevention and treatment should be sensitive to underlying socioeconomic and environmental contributions as well as factors that reduced access to adequate healthcare and good nutrition.
Impact of Diet on Kidney Stones
When the subject of urolithiasis and diet comes up, recommendations about the intake of calcium, oxalates, and hydration cannot be avoided. However, the reality is that we should be looking at broader considerations when it comes to the integrative approach to kidney stone prevention.
Consumption of the standard American diet (SAD) seems to increase the risk of kidney stone formation. SAD includes the consumption of sugary beverages and soda, as well as elevated intake of processed foods and animal protein. Interestingly, eating more fresh produce is protective. This is associated with the nutritional benefit, including (but not limited to) foods rich in potassium magnesium, and fiber. Furthermore, taking vitamin D, and good hydration risk were reversed.
This topic deserves a deeper dive, and we do so in another blog [found here].
Genetics and Kidney Stones
There seems to be a familial link when it comes to the development of kidney stones. Recently, genome-wide association studies uncovered several genetic sequence variants (SNPs) that lead to an increased risk of kidney stone development. Single nucleotide polymorphisms (SNPs) have been associated with kidney stones including those found in CLDN14, ALPL, SLC34A1, CASR, VDR, OPN, and TRPV5.
These genes play a role in the way the kidney handles certain vitamins and minerals including vitamin D, calcium, and phosphate. Imbalances of these nutrients are involved in the pathophysiology of stone formation, therefore stands to reason that genetic variations that result in mishandling will increase the risk. There is still a lot more to learn about the contribution of genetic factors to stone formation. However, what we do know is that we can modulate these risks through environmental and dietary modification.
Microbiome and Kidney Stones
Balance of the gut bacteria also plays an important role in causing or preventing kidney stones. The most studied organism is Oxalobacter formigenes, which has been found to be protective when present in adequate quantities as part of the GI microflora. This bacterium degrades oxalate in the gut decreasing its absorption and excretion in the urine.
In addition, dysbiosis in general is linked to kidney stone formation in those people prone to stone formation due to genetic or environmental factors. Therefore (and unsurprisingly), gut health is an important consideration when addressing kidney stones. Antibiotics which negatively alter the gut microbiome, are linked to higher rates of kidney stones.
More on the contribution of the microbiome on kidney stone formation will be the topic of another blog on the gut-kidney access here.
The Bottom Line
Although genetic factors may impact risk of kidney stone formation, environmental, dietary, as well as factors affecting the integrity of the gut microbiome play a large role in turning on those genes and impacting stone formation. Therefore, the integrative approach to addressing kidney stones must account for a combination of all these factors and practitioners should formulate and personalized approach that modifies relevant lifestyle factors.
This blog was written with contributions from Lara Zakaria, RPh MS CNS CDN IFMCP
The post Kidney Stones: The Integrative Approach to Prevention and Management appeared first on Integrative Kidney.]]>