
3 years of lifestyle interventions improved exercise capacity and decreased the losses in neuromuscular and cardiorespiratory fitness in CKD patients
In this study, researchers randomized 161 patients with stage 3-4 CKD to either get usual care or usual care plus lifestyle “intervention” for 3 years.
The lifestyle intervention comprised of care from a multidisciplinary team, including a nephrologist, nurse practitioner, exercise physiologist, dietitian, diabetes educator, psychologist, and social worker.
The patients were coached for 8 weeks and then followed for 34 months with a home-based program.
The study did not look at the progression of CKD but it found that a 3-year lifestyle intervention doubled the percentage of CKD patients meeting physical activity guidelines, improved exercise capacity, and decreased the losses in neuromuscular and cardiorespiratory fitness.
It appears that the study mainly focused on exercise. So imagine the benefit of a comprehensive lifestyle modification plan that includes nutrition, exercise, stress management, sleep improvement, and attention to toxin exposure and gut-kidney connection. That’s what we focus on.
Join us in the fight against kidney disease and receive the FREE Report “5 Pitfalls to Avoid When Caring for Kidney Patients”
Curcumin powder did not improve markers of vascular dysfunction in PKD
This is essentially a negative study.
It demonstrated that Curcumin powder did not improve markers of vascular dysfunction in children and young adults with PKD. The study was conducted for only one year using a dose of 25 mg/kg per day of curcumin.
This is a classic supplement or nutrient study that is usually underpowered or conducted for short periods of time for a disease that takes years or even decades to evolve. Nevertheless, the study proved that short-term use of curcumin is not beneficial for vascular health for young patients with polycystic kidney disease.
Low serum zinc levels were associated with infections in CKD patients
This did not really need research but it is now studied and it is official: Low zinc levels in patients with CKD lead to infection (..well among other things).
This retrospective study analyzed data from 299 CKD patients who had serum zinc levels checked to evaluate anemia. They used the level of 50 mcg/dl as the cutoff between low or “high” zinc values.
Low serum zinc values remained an independent risk factor for infection-related hospitalization. This was especially true for patients taking proton pump inhibitors (PPIs) medications.
Read about the effect of Zinc on kidney health in this blog.
Download Your Copy!






Join here to receive FREE monthly update on the latest research in Integrative Nephrology straight to your inbox.
We would love to here your feedback. Let us know what you think of these educational materials and if you like us to focus on certain topics. Email us at info@inkidney.com
The post January Research and News appeared first on Integrative Kidney.]]>Polycystic kidney disease (PKD) is the most common inherited kidney disease affecting one in 800 people. There have been several advances in our understanding of PKD since our last blog. In a previous blog, we discussed the genetics of PKD and how genetic variants translate into a disease. In this blog, we will discuss recommendations for water, salt, and caffeine intake to reduce cyst growth. You will find out if ketogenic diet or intermittent fasting is the best diet for polycystic kidney disease.
PKD at the Cellular Level
To determine the best PKD diet and lifestyle recommendations, we must understand what is happening at the cellular level. In essence, abnormalities in PC1 or PC2 proteins will activate two pathways inside the cell. First, it activates the cAMP pathway which regulates fluid transport. Second, it changes the way cells make energy from sugar (called glycolysis). When PC1 or PC2 proteins don’t work well, they switch from aerobic (with oxygen) to anaerobic (without oxygen) glycolysis. This is similar to the shift that occurs in cancer cells.
While anaerobic glycolysis produces less energy from glucose, it is faster than aerobic glycolysis. This faster energy production allows the cells to grow faster. However, it also leads to a critical dependence on glucose.1
How Much Water to Drink in PKD
Vasopressin, also called anti-diuretic hormone (ADH), is a hormone that is produced by the brain and excreted by the pituitary gland. It plays an important role in the body’s fluid and sodium balance, blood pressure, and kidney function. ADH was found in several studies to promote cyst growth by stimulating the production of cAMP. Further proving the role of ADH in polycystic kidney disease, cyst growth was inhibited in both forms of PKD by administering ADH receptor blockers (medications that block ADH).
Dehydration can increase ADH and make cysts worse. Drinking large amounts of water leads to a significant decrease in the progression of PKD. The optimal amount of water to drink in PKD patients depends on the amount of salt and food they eat. The simplest way to assess this is by checking a 24-hour urine osmolality. You can use our calculator to assess the amount of water you should drink daily based on your 24-hour urine osmolality. Alternatively, measuring first morning urine osmolality can be used. The target for that is keeping the level less than 280 mOsm/kg.
In addition to dehydration, other factors that lead to the production of ADH include stress, pain, and surgery. These factors, therefore, can indirectly lead to cyst growth and further harm kidney function.
Download Your Copy!
Polycystic Kidney Disease and Caffeine
In the laboratory, caffeine increased cAMP accumulation in the cells. Yet, in human clinical trials, caffeine intake was not directly associated with kidney size in patients with PKD. An analysis in one clinical trial found no significant association between the consumption of caffeine from coffee and tea on the progression of ADPKD.
Join us in the fight against kidney disease and receive the FREE Report “5 Pitfalls to Avoid When Caring for Kidney Patients”
Calorie-restricted and Keto Diets for Polycystic Kidney Disease
Kidney cysts thrive on sugar or glucose, as discussed earlier. Therefore, calorie-restricted and ketogenic diets can be beneficial for patients with PKD. Ketogenic diets induce a state that resembles starvation by providing high fat content and low protein and carbohydrate content. Time-restricted feeding such as intermittent fasting can have similar effects. Studies on animals demonstrated that ketosis could decrease cyst growth in PKD. These effects were thought to be mediated by a strong inhibition of mTOR.2
It is worth mentioning here that metformin can activate AMPK and is currently being studied in PKD.
To our knowledge, there is no published human study to confirm the effect of ketogenic diets and intermittent fasting on PKD. However, given the strong benefit of ketosis on cyst growth, we generally recommend a plant-based ketogenic diet or intermittent fasting in addition to a large water intake for patients with PKD.
Dietary, Lifestyle, and Water Recommendations for PKD
The phrase “our genes are not our destiny” describes how nutrition and lifestyle factors can have a positive impact on genetic expression for certain diseases. Drinking large amounts of filtered water, restricting salt intake, a ketogenic diet, or intermittent fasting can have significant benefits in patients with PKD. So far, limiting caffeine is not necessary to improve PKD, but it has other health benefits. Finally, stress reduction techniques can help to lower ADH and reduce kidney cysts.
Ongoing Studies of Diet and Lifestyle PKD Treatments
- PREVENT-ADPKD trial is looking at water intake and the progression of ADPKD. It should be released in late 2021.
- DRINK trial is investigating water intake in ADPKD. It should also be released in late 2021 or early 2022.
- METROPOLIS trial is comparing Metformin and Tolvaptan for the treatment of ADPKD. It should be completed in early 2022.
- Time-restricted feeding in ADPKD is currently recruiting subjects and is estimated to be completed by end of 2022.
- Keto-ADPKD trial is looking at how the ketogenic diet affects the progression of ADPKD. It should be completed in mid-2022.
- Curcumin Therapy to treat vascular dysfunction in ADPKD was completed in late 2020. It should be released soon.
1 It is noteworthy that glycolysis is inhibited by a cellular messenger called AMP-activated protein kinase (AMPK). It is activated by another messenger called mTOR. Metformin activates AMPK.
2 Activation of AMPK and inhibition of mTOR can theoretically inhibit glycolysis in cells that line the cysts in PKD. However, studies that looked at medications that inhibit mTOR such as sirolimus, did not show any benefit in PKD.
The post Diet and Lifestyle Modifications in PKD appeared first on Integrative Kidney.]]>

Hereditary Kidney Disease: The Genetics of PKD
PKD is a group of two genetic disorders that affect the kidneys and cause the formation of multiple fluid-filled cysts of various sizes. As these cysts grow, they squeeze and destroy normal kidney tissue, eventually leading to loss of kidney function. PKD is an inherited disease, meaning it’s passed down genetically from parent to child, just like eye or hair color. Polycystic kidney disease can be autosomal-dominant (ADPKD) affecting 50% of offspring. Or it can be autosomal-recessive (ARPKD), affecting 25% of offspring.
Mutations in one of two genes (PKD1 or PKD2) account for most cases of ADPKD. Polycystic kidney disease 1 gene (PKD1) mutations are the most common. About 80 percent of patients affected by ADPKD have a PKD1 mutation. PKD2 gene is the cause of up to 20% of ADPKD cases and it is usually associated with milder course.
The PKD1 and PKD2 genes provide the blueprints for important kidney and liver proteins called polycystin-1 (PC1) and polycystin-2 (PC2). These proteins are crucial for the structure of the kidney’s tubular cells, which filter and clean the blood. PC1 and PC2 influence healthy growth and fluid secretion in these cells. However, in people with hereditary kidney disease, abnormal genetic blueprints lead to the production of abnormal proteins. When these kidney proteins don’t work properly, cysts accumulate and damage the kidney.
Cysts that form in polycystic kidney disease usually occur when the cells lining the tubules of the kidney start growing out of control (called proliferation). These outgrowths bulge and eventually separate into cysts. As the cysts grow, they transport fluid across their lining, forming a fluid-filled sack much like a balloon. So, when we think about PKD, we should remember two processes: cell proliferation (cell growth) and fluid secretion into the cysts.
Truncating vs. Non-truncating mutations
Sometimes a change in the DNA sequence of a gene results in the creation of an “early stop.” This early stop functions to end the translation of the gene into a protein in our cell factory. This produces a shortened or truncated protein. This type of variant can have serious functional consequences. They are called truncating mutations.
The relationship between genetic variants and prognosis in PKD is not completely understood. In a study that looked at the “renal survival” in 741 patients with ADPKD, PKD2 mutations were associated with approximately 20 years longer survival than PKD1 mutations. In addition, the type of PKD1 mutation, not its position, correlated strongly with renal survival. The median age at onset of kidney failure was 55 years for carriers of a truncating mutation and 67 years for carriers of a non-truncating mutation. This observation allows the integration of genic and allelic effects into a single scheme, which may have prognostic value.
This points to the importance of genetic testing even in a genetic disease with an obvious clinical presentation such as PKD. Identifying patients with truncating mutations may help selecting those who require more aggressive therapies.
PKD at the Cellular Level
To determine the best PKD diet and lifestyle recommendations, we must understand what is happening at the cellular level. In essence, abnormalities in PC1 or PC2 proteins will activate two pathways inside the cell. First, it activates the cAMP pathway which regulates fluid transport. Second, it changes the way cells make energy from sugar (called glycolysis). When PC1 or PC2 proteins don’t work well, they switch from aerobic (with oxygen) to anaerobic (without oxygen) glycolysis. This is similar to the shift that occurs in cancer cells.
While anaerobic glycolysis produces less energy from glucose, it is faster than aerobic glycolysis. This faster energy production allows the cells to grow faster. However, it also leads to a critical dependence on glucose.1
In the next blog we will discuss the 2021 update about diet and Lifestyle Treatments to Improve Polycystic Kidney Disease (PKD).
1 It is noteworthy that glycolysis is inhibited by a cellular messenger called AMP-activated protein kinase (AMPK). It is activated by another messenger called mTOR. Metformin activates AMPK.
The post Polycystic Kidney Disease Genetics appeared first on Integrative Kidney.]]>
What is Polycystic Kidney Disease?
PKD is a group of two genetic disorders that affects the kidneys and cause the formation of multiple fluid-filled cysts of various sizes. As these cysts grow, they squeeze and destroy normal kidney tissue, eventually leading to loss of kidney function. PKD is a Mendelian inherited disease, meaning it’s passed down genetically like eye or hair color. It said to be autosomal-dominant, slowly progressive disease affecting 50% of offspring, or autosomal-recessive which affect 25% of offspring of affected individuals but is usually rapidly progressive in childhood.
How does PKD develop?
Cysts that form in PKD usually occur when the cells lining the tubules of the kidney end up proliferating causing outpouchings (bulgings) that eventually separate into cysts. These cysts end up growing, transporting fluid across their lining into their lumen forming a fluid-filled sack or balloon. So, when we think about PKD, we should remember two processes: cell proliferation (cell growth) and fluid secretion into the cysts.
So, when we think about PKD, we should remember two processes: cell proliferation (cell growth) and fluid secretion into the cysts.
Share on X
In this blog, we focus on factors that affect fluid secretion into the cysts. This process is mediated by a cellular messenger called cyclic adenosine monophosphate, or cAMP, which is activated by the actions of anti-diuretic hormone (ADH). It should be noted that it can also be activated by other hormones such as the parathyroid hormone, prostaglandin E2, epinephrine, among others, however we will focus on ADH.
What is ADH?
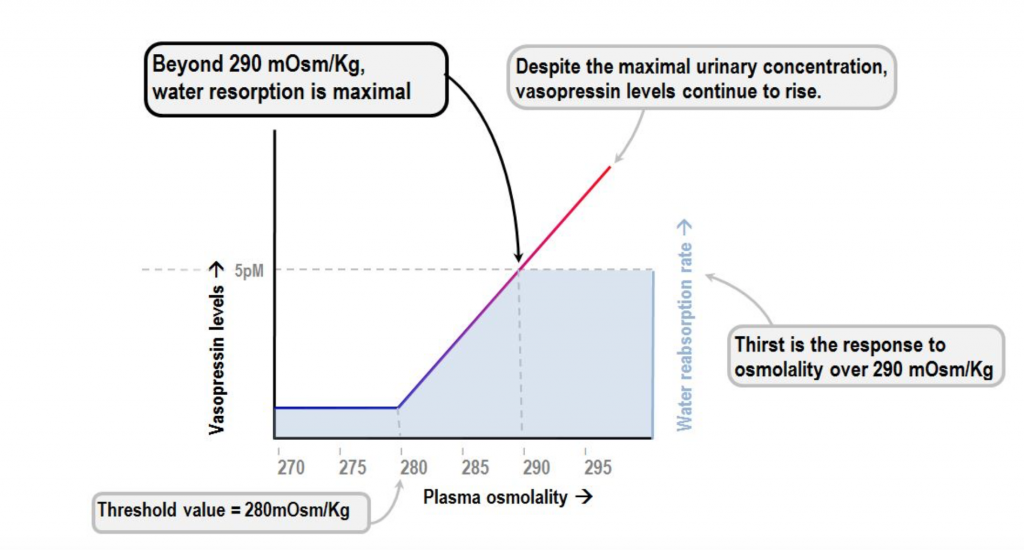
ADH (also known as vasopressin) is a hormone produced by the brain and excreted by the pituitary gland. The purpose of ADH is to tightly regulate water balance and osmotic pressure. The presence of this hormone is crucial for survival, it is what gives humans and other land-dwelling animals the ability to survive out of the water.
When the body’s receptor’s sense that there’s an accumulation of certain solutes such as sodium, a chain of events occurs to preserve water (fluid retention). The chain of events is triggered by an increase in ADH. The kidneys have receptors that respond to ADH by formation of cAMP which leads to increase water retention.
Sodium concentration in the blood is reflective of the amount of water in our body. High sodium (and osmolality) levels stimulate the production of ADH and preservation of water. Low sodium levels inhibit the production of ADH stimulating water release. In fact, at a certain low level of sodium concentration and osmolality ADH excretion will be shut off completely.
Sodium concentration in the blood is reflective of the amount of water in our body. High sodium levels stimulate the production of ADH and preservation of water.
Share on X
The role of ADH in PKD
ADH was found in several studies to promote cyst growth by stimulating the production of cAMP. Drinking large amounts of water to a degree that the urine osmolality is lower than serum osmolality leads to a significant decrease in the progression of PKD. Cyst growth was inhibited in both forms of PKD by administering ADH receptor blockers. In addition to dehydration, other factors that lead to the production of ADH include stress, pain, and surgery. These factors, therefore, can indirectly lead to cyst growth and further decline in kidney function.
Researchers found that drinking large amounts of water lead to significant decrease in the progression of PKD.
Share on X
What can you do if you have PKD?
The integrative approach to PKD focuses on drinking adequate amounts of filtered water. In general, we recommend that kidney patients who have no significant volume overload problems drink half of their body weight in ounces of water daily. So, for example if you weigh 190 lbs., aim to drink at least 95 oz of water daily. Patients with PKD should aim to have their water intake at the highest end and restrict their salt intake to decrease serum osmolality and ADH excretion.
Yoga and stress reduction techniques, such as meditation or breathing exercises, can also play an important role in inhibiting ADH excretion and other hormones that can activate cAMP such as epinephrine.
In addition, assuring adequate intake of high-quality vitamin D will help inhibit Parathyroid hormone (PTH – another hormone that influences cAMP production) and limit cyst growth.
Finally, there are foods and beverages that can lead to accumulation of cAMP by inhibiting an enzyme called phosphodiesterase (PDE). In certain conditions such as heart disease, some of these same foods may benefit, however they should be avoided by PKD patients to preserve PDE function and minimize cAMP. These include methylxanthines such as caffeine, found in coffee, mate, tea, and cacao. In addition, catechins found in green tea, and flavonoids found in red wine should be avoided. Some recent laboratory studies suggest that extracts of artichoke and ginger might also be contraindicated in PKD, but more research should be done to draw any conclusive outcomes.
As always, we recommend that you discuss these lifestyle recommendations for polycystic kidney disease with your provider or nephrologist since every kidney patient is unique.
The post Lifestyle Modifications for Polycystic Kidney Disease appeared first on Integrative Kidney.]]>