What is Polycystic Kidney Disease?
PKD is a group of two genetic disorders that affects the kidneys and cause the formation of multiple fluid-filled cysts of various sizes. As these cysts grow, they squeeze and destroy normal kidney tissue, eventually leading to loss of kidney function. PKD is a Mendelian inherited disease, meaning it’s passed down genetically like eye or hair color. It said to be autosomal-dominant, slowly progressive disease affecting 50% of offspring, or autosomal-recessive which affect 25% of offspring of affected individuals but is usually rapidly progressive in childhood.
How does PKD develop?
Cysts that form in PKD usually occur when the cells lining the tubules of the kidney end up proliferating causing outpouchings (bulgings) that eventually separate into cysts. These cysts end up growing, transporting fluid across their lining into their lumen forming a fluid-filled sack or balloon. So, when we think about PKD, we should remember two processes: cell proliferation (cell growth) and fluid secretion into the cysts.
So, when we think about PKD, we should remember two processes: cell proliferation (cell growth) and fluid secretion into the cysts.
Share on X
In this blog, we focus on factors that affect fluid secretion into the cysts. This process is mediated by a cellular messenger called cyclic adenosine monophosphate, or cAMP, which is activated by the actions of anti-diuretic hormone (ADH). It should be noted that it can also be activated by other hormones such as the parathyroid hormone, prostaglandin E2, epinephrine, among others, however we will focus on ADH.
What is ADH?
ADH (also known as vasopressin) is a hormone produced by the brain and excreted by the pituitary gland. The purpose of ADH is to tightly regulate water balance and osmotic pressure. The presence of this hormone is crucial for survival, it is what gives humans and other land-dwelling animals the ability to survive out of the water.
When the body’s receptor’s sense that there’s an accumulation of certain solutes such as sodium, a chain of events occurs to preserve water (fluid retention). The chain of events is triggered by an increase in ADH. The kidneys have receptors that respond to ADH by formation of cAMP which leads to increase water retention.
Sodium concentration in the blood is reflective of the amount of water in our body. High sodium (and osmolality) levels stimulate the production of ADH and preservation of water. Low sodium levels inhibit the production of ADH stimulating water release. In fact, at a certain low level of sodium concentration and osmolality ADH excretion will be shut off completely.
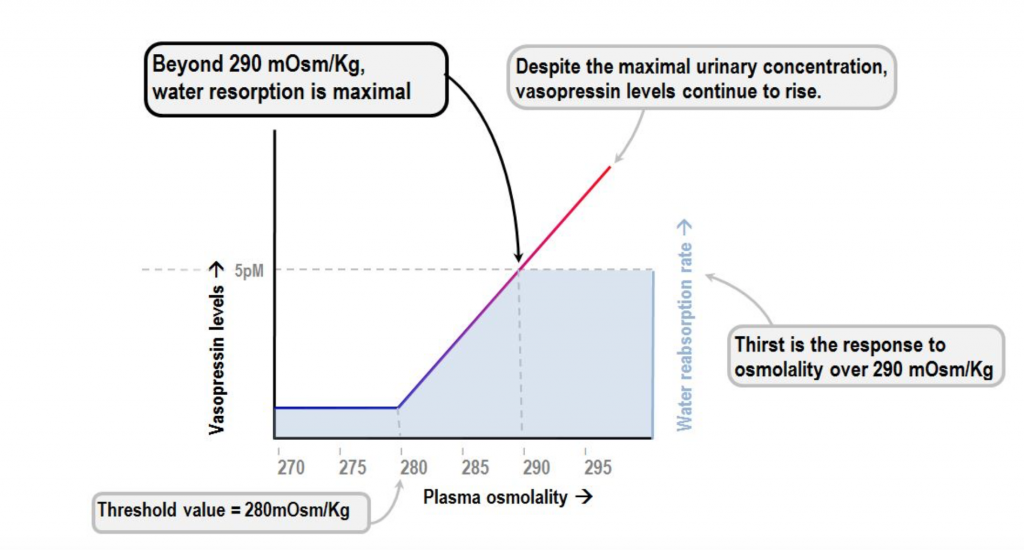
Sodium concentration in the blood is reflective of the amount of water in our body. High sodium levels stimulate the production of ADH and preservation of water.
Share on X
The role of ADH in PKD
ADH was found in several studies to promote cyst growth by stimulating the production of cAMP. Drinking large amounts of water to a degree that the urine osmolality is lower than serum osmolality leads to a significant decrease in the progression of PKD. Cyst growth was inhibited in both forms of PKD by administering ADH receptor blockers. In addition to dehydration, other factors that lead to the production of ADH include stress, pain, and surgery. These factors, therefore, can indirectly lead to cyst growth and further decline in kidney function.
Researchers found that drinking large amounts of water lead to significant decrease in the progression of PKD.
Share on X
What can you do if you have PKD?
The integrative approach to PKD focuses on drinking adequate amounts of filtered water. In general, we recommend that kidney patients who have no significant volume overload problems drink half of their body weight in ounces of water daily. So, for example if you weigh 190 lbs., aim to drink at least 95 oz of water daily. Patients with PKD should aim to have their water intake at the highest end and restrict their salt intake to decrease serum osmolality and ADH excretion.
Yoga and stress reduction techniques, such as meditation or breathing exercises, can also play an important role in inhibiting ADH excretion and other hormones that can activate cAMP such as epinephrine.
In addition, assuring adequate intake of high-quality vitamin D will help inhibit Parathyroid hormone (PTH – another hormone that influences cAMP production) and limit cyst growth.
Finally, there are foods and beverages that can lead to accumulation of cAMP by inhibiting an enzyme called phosphodiesterase (PDE). In certain conditions such as heart disease, some of these same foods may benefit, however they should be avoided by PKD patients to preserve PDE function and minimize cAMP. These include methylxanthines such as caffeine, found in coffee, mate, tea, and cacao. In addition, catechins found in green tea, and flavonoids found in red wine should be avoided. Some recent laboratory studies suggest that extracts of artichoke and ginger might also be contraindicated in PKD, but more research should be done to draw any conclusive outcomes.
As always, we recommend that you discuss these lifestyle recommendations for polycystic kidney disease with your provider or nephrologist since every kidney patient is unique.
The post Lifestyle Modifications for Polycystic Kidney Disease appeared first on Integrative Kidney.]]>